The key to reducing the morbidity and mortality associated with skin cancers is prevention and early detection. Healthcare professionals involved in the care of adults and children are in a unique position to routinely evaluate patients for skin cancer as well as to educate their patients about self-examination and preventive measures. This course provides an overview of the various types of nonmelanoma and melanoma skin cancers, including a description of the populations at high risk for these cancers and the criteria for distinguishing between benign and malignant melanomas. The course also includes details on diagnostic techniques, treatment options, prognosis, and follow-up care. The importance of patient education pertaining to proper preventive measures and the current recommendations concerning screening are also highlighted.
This course is designed for physicians, physician assistants, nurses, and other healthcare providers seeking to enhance their knowledge about the prevention, screening, diagnosis, and treatment of nonmelanoma skin cancers and melanoma.
The purpose of this course is to enhance knowledge about the clinical presentation of skin cancers in order to help primary healthcare providers detect skin cancer and make appropriate referrals early, when treatment is most successful.
Upon completion of this course, you should be able to:
- Describe the etiology and epidemiology of skin cancers.
- Discuss the role of UV radiation in the development of nonmelanomas and melanomas.
- Describe the clinical features, treatment, and prognosis of basal cell carcinomas and squamous cell carcinomas.
- Describe the clinical features, treatment, and appropriate follow-up care of melanoma.
- Outline skin cancer screening guidelines.
- Discuss effective preventive measures for skin cancers, including resources to educate patients about skin cancers and prevention.
Lori L. Alexander, MTPW, ELS, MWC, is President of Editorial Rx, Inc., which provides medical writing and editing services on a wide variety of clinical topics and in a range of media. A medical writer and editor for more than 30 years, Ms. Alexander has written for both professional and lay audiences, with a focus on continuing education materials, medical meeting coverage, and educational resources for patients. She is the Editor Emeritus of the American Medical Writers Association (AMWA) Journal, the peer-review journal representing the largest association of medical communicators in the United States. Ms. Alexander earned a Master’s degree in technical and professional writing, with a concentration in medical writing, at Northeastern University, Boston. She has also earned certification as a life sciences editor and as a medical writer.
Contributing faculty, Lori L. Alexander, MTPW, ELS, MWC, has disclosed no relevant financial relationship with any product manufacturer or service provider mentioned.
John M. Leonard, MD
Mary Franks, MSN, APRN, FNP-C
The division planners have disclosed no relevant financial relationship with any product manufacturer or service provider mentioned.
Sarah Campbell
The Director of Development and Academic Affairs has disclosed no relevant financial relationship with any product manufacturer or service provider mentioned.
The purpose of NetCE is to provide challenging curricula to assist healthcare professionals to raise their levels of expertise while fulfilling their continuing education requirements, thereby improving the quality of healthcare.
Our contributing faculty members have taken care to ensure that the information and recommendations are accurate and compatible with the standards generally accepted at the time of publication. The publisher disclaims any liability, loss or damage incurred as a consequence, directly or indirectly, of the use and application of any of the contents. Participants are cautioned about the potential risk of using limited knowledge when integrating new techniques into practice.
It is the policy of NetCE not to accept commercial support. Furthermore, commercial interests are prohibited from distributing or providing access to this activity to learners.
Supported browsers for Windows include Microsoft Internet Explorer 9.0 and up, Mozilla Firefox 3.0 and up, Opera 9.0 and up, and Google Chrome. Supported browsers for Macintosh include Safari, Mozilla Firefox 3.0 and up, Opera 9.0 and up, and Google Chrome. Other operating systems and browsers that include complete implementations of ECMAScript edition 3 and CSS 2.0 may work, but are not supported. Supported browsers must utilize the TLS encryption protocol v1.1 or v1.2 in order to connect to pages that require a secured HTTPS connection. TLS v1.0 is not supported.
The role of implicit biases on healthcare outcomes has become a concern, as there is some evidence that implicit biases contribute to health disparities, professionals' attitudes toward and interactions with patients, quality of care, diagnoses, and treatment decisions. This may produce differences in help-seeking, diagnoses, and ultimately treatments and interventions. Implicit biases may also unwittingly produce professional behaviors, attitudes, and interactions that reduce patients' trust and comfort with their provider, leading to earlier termination of visits and/or reduced adherence and follow-up. Disadvantaged groups are marginalized in the healthcare system and vulnerable on multiple levels; health professionals' implicit biases can further exacerbate these existing disadvantages.
Interventions or strategies designed to reduce implicit bias may be categorized as change-based or control-based. Change-based interventions focus on reducing or changing cognitive associations underlying implicit biases. These interventions might include challenging stereotypes. Conversely, control-based interventions involve reducing the effects of the implicit bias on the individual's behaviors. These strategies include increasing awareness of biased thoughts and responses. The two types of interventions are not mutually exclusive and may be used synergistically.
#90774: Skin Cancers
Approximately 5.4 million nonmelanoma skin cancers among 3.3 million people are diagnosed each year, making it the most common cancer in the United States [1,2]. The cost of treating skin cancers is estimated at $8.1 billion each year [2]. The two most frequently occurring nonmelanoma skin cancers are basal cell carcinoma and squamous cell carcinoma, and the prevalence of these two skin cancers has been increasing worldwide. Since the 1980s, the incidence of squamous cell carcinoma has increased 3% to 10% each year, and the incidence of basal cell carcinomas has increased by as much as 80% [2,3,200,201]. The third most common skin cancer, melanoma, is the fifth leading type of cancer diagnosed in both men and women in 2025, accounting for 1% of all skin cancers but the majority of deaths; an estimated 104,960 new cases of invasive and 107,240 cases of in situ melanoma will be diagnosed in 2025 [1]. The prevalence of melanoma has increased at a rate faster than any other malignant disease, with slightly greater increases among men compared with women [4,202]. Due to these increases, skin cancer will develop in one of five Americans during his or her lifetime [2,5,6]. However, data indicate that, among individuals younger than 50 years of age, the incidence of invasive melanoma appears to be declining at a rate of 1% per year among men and has stabilized among women; among individuals 50 years of age or older, the incidence appears to have plateaued [1].
The reason for the dramatic increases in these three types of skin cancers is thought to be related to increased exposure to the sun through outdoor recreation beginning in childhood. It has been estimated that nearly 90% of nonmelanoma skin cancers can be attributed to exposure to ultraviolet (UV) rays, especially UV-B rays [6,203]. Thus, many cases of nonmelanoma and melanoma could be avoided through appropriate behavioral changes [6].
This course provides an overview of skin cancers, with a description of the various types of skin cancers and the demographic variations in their incidences and mortality rates. The role of UV radiation in the development of skin cancers is discussed, as are other risk factors for nonmelanomas and melanoma. The focus of the course is on the detection, diagnosis, treatment, prognosis, and follow-up for basal cell and squamous cell carcinomas and melanoma. Also addressed in detail are guidelines for screening and the importance of patient education in preventing skin cancers.
A wide variety of tumors and lesions arise in the skin, and most are benign. However, it is important to evaluate all suspicious lesions to distinguish benign tumors from nonmelanomas and melanomas. Skin cancers primarily comprise melanoma and two types of nonmelanomas—basal cell carcinoma and squamous cell carcinoma. Basal cell carcinoma is far more common, accounting for approximately 70% to 80% of nonmelanoma skin cancers, while squamous cell carcinoma accounts for nearly 20% [7,8].
Several less common types of skin cancers together account for less than 1% of nonmelanoma skin cancers [9]. These cancers include Kaposi sarcoma, adnexal tumors, cutaneous lymphoma, sarcomas, and Merkel cell carcinoma.
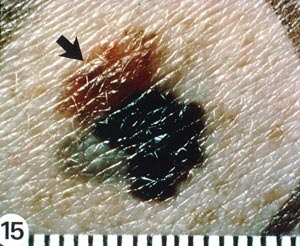
Kaposi sarcoma (Image 1 and Image 2) became more common with the introduction of the human immunodeficiency virus (HIV) and acquired immunodeficiency syndrome (AIDS) but has become rare again as a result of treatment of these conditions with protease inhibitors [10]. Most adnexal tumors, which originate in the hair follicles or sweat glands, are benign. Lymphomas and sarcomas usually originate in lymph nodes, viscera, and connective tissue but develop in the skin on rare occasions. Cutaneous T-cell lymphoma (mycosis fungoides) is the most common primary cutaneous lymphoma, while dermatofibrosarcoma protuberans and angiosarcoma are among the various types of sarcomas that arise from the skin. Merkel cell carcinoma arises from neuroendocrine cells in the skin, and the estimated incidence is 0.7 cases per 100,000 people; however, the incidence appears to be rising [11,12,13,14]. As with basal cell carcinoma and squamous cell carcinoma, Merkel cell carcinoma is caused in part by exposure to the sun and is found on the head or neck in about half of cases and on the extremities in about 40% of cases [11,14]. Unlike the other nonmelanomas, Merkel cell carcinoma is aggressive and has a strong tendency to recur, to spread to regional lymph nodes, and to metastasize [15].


Melanomas occur less frequently than nonmelanoma skin cancers, but they are associated with greater morbidity and mortality due to their propensity to metastasize. Melanomas account for approximately 1% of all skin cancers, but for approximately 65% of all deaths related to skin cancers [1,2,23].
The risk for skin cancers varies among several populations defined by sex, age, ethnicity, comorbid conditions, and geographic location. It is difficult to know the true incidence of nonmelanomas, as they are not documented in cancer registries, as melanoma is. In an early attempt to determine the incidence, researchers studied approximately 10 million people in four geographic regions of the United States (Dallas/Ft. Worth, Minneapolis/St. Paul, Iowa, and San Francisco/Oakland) in the early 1970s and found that 300,000 cases of nonmelanoma skin cancer were diagnosed in a six-month period [16].
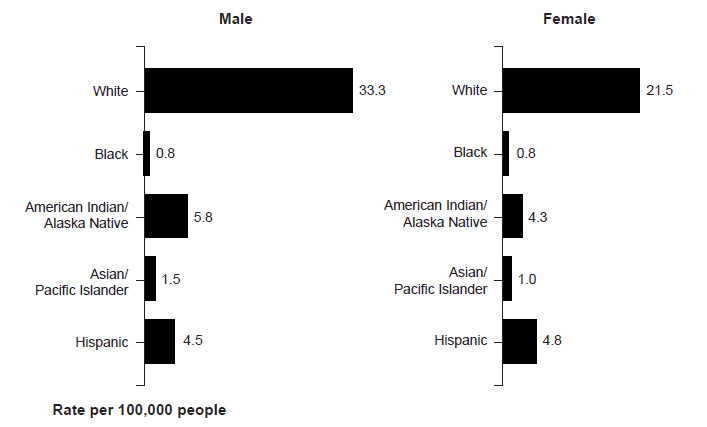
Nonmelanoma skin cancers are more common in men, with squamous cell carcinoma affecting two to three times as many men as women and basal cell carcinoma occurring at a ratio of 3:2 (men to women) [17,18]. Melanoma also occurs more frequently in men. The American Cancer Society estimates that, in 2025, an estimated 65,740 cases of melanoma will be diagnosed in men and 46,950 cases in women [1]. The incidence of melanoma is higher among men across most racial/ethnic populations (Figure 1) [19].
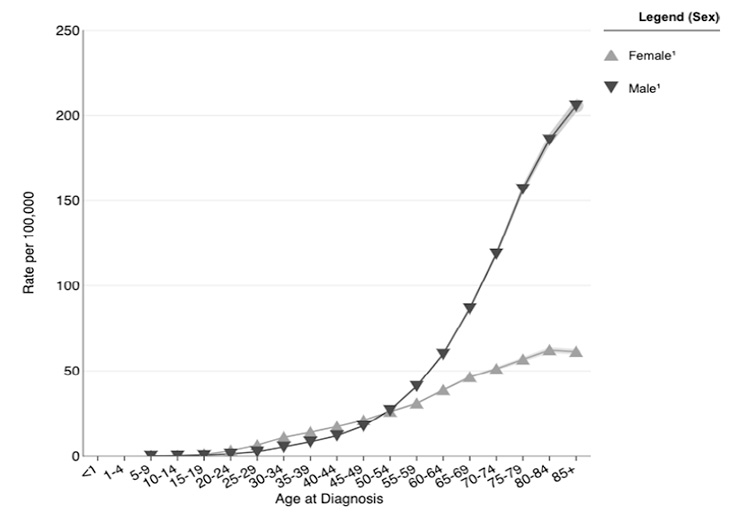
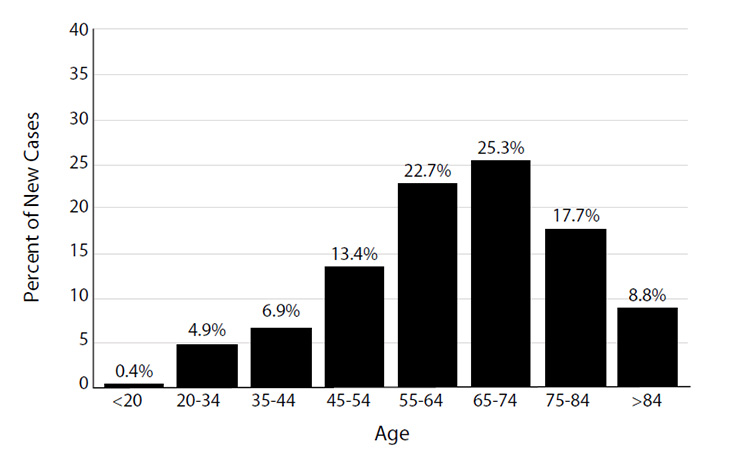
Because most cases of skin cancer are linked to sun exposure, the incidence increases with age [2,17]. Similarly, the incidence of melanoma steadily increases after age 19 years, peaking at 205.6 per 100,000 population for men older than 85 years of age and 62.1 per 100,000 population for women 80 to 84 years of age (Figure 2) [20]. The median age at the time of diagnosis of cutaneous melanoma was 66 years in 2017–2021 (Figure 3) [21]. The age and sex distribution of melanoma among children and adolescents differs from that among adults. Between 2017 and 2021, the rate of melanoma among individuals 1 to 19 years of age was 0.28 per 100,000 (0.22 per 100,000 in boys and 0.34 per 100,000 in girls) [22].
The incidences of specific types of skin cancer vary according to race/ethnicity, and the risk is more than 20 times higher for the White population than for populations with darker skin, such as Black, American Indian/Alaska Native, Hispanic, and Asian/Pacific Islander populations [9,23]. This large disparity is the result of the photoprotection provided by increased melanin in the epidermis of individuals with darker skin, which can filter up to twice as much UV radiation than the epidermis of White individuals [25,26].
As is true for the White population, basal cell carcinoma is the most common skin cancer among the Hispanic and Asian populations [27,28]. In fact, among Hispanic individuals, basal cell carcinoma is six times more likely than squamous cell carcinoma [28]. In contrast, squamous cell carcinoma is the most common skin cancer in the Black population [25,28]. Melanoma is the third most common skin cancer among all racial/ethnic populations [25,28]. The highest rate of melanoma is found among non-Hispanic White men and the lowest is among Black women [29,202]. Although melanoma is predominant among White men compared with White women, the incidence of melanoma in men and women is similar in Black, Hispanic, and Asian/Pacific Islander populations [29,202]. The clinical features of skin cancers (i.e., appearance and anatomic site) also vary according to race/ethnicity, as will be discussed later.
The risk of skin cancer is also influenced by comorbid or previous conditions. One substantial risk factor is a compromised immune system (because of either drugs or disease). Due to immunosuppression, skin cancers develop in 30% to 70% of patients who have a transplanted organ, with a 100-fold increased risk for developing squamous cell carcinoma, a 24-fold increased risk for Merkel cell carcinoma, a 6-fold increased risk for basal cell carcinoma, and a 2-fold increased risk for melanoma [9,30,134]. The prevalence of skin cancers is also high among individuals infected with HIV, and lesions in this population tend to be more aggressive [9,30]. A higher risk of squamous cell carcinoma is significantly associated with seropositivity for human papillomavirus (HPV) types 16 and 18, but a direct causal relationship has not been established [31]. In addition, individuals with a history of skin cancer are at increased risk for another skin cancer, and survivors of childhood cancers are at increased risk for nonmelanoma skin cancers, primarily basal cell carcinoma, particularly in an anatomic site that had been treated with radiation therapy [9,32,33,34,205].
Geographic area of residence also plays a role in the risk of melanoma, with a higher risk for individuals who live near the equator, where the sun's rays are most intense [9,35].
As noted, the incidence of all types of skin cancers in adults has been increasing over the past few decades. In 1930, the likelihood of melanoma was 1 in 5,000 Americans; by 2018–2021, that rate increased to 1 in 29 for men and 1 in 40 for women [1,36]. Overall, the rate of skin cancers has increased 3% to 8% per year since the 1960s [37]. In addition, the incidence of pediatric melanoma increased at a rate of 2% to 2.9% per year since the 1970s [38]. As discussed, the most recent data show melanoma rates may be leveling off or even decreasing [1]. The demographics of other skin cancers are also changing. Both basal cell and squamous cell carcinoma are occurring in an increasing percentage of people younger than 40 years of age, and one study found a disproportionate increase in basal cell carcinoma among women in that age-group [39,201]. These two types of skin cancer have nearly tripled in frequency among women younger than 40 years of age since the 1970s [9,40].
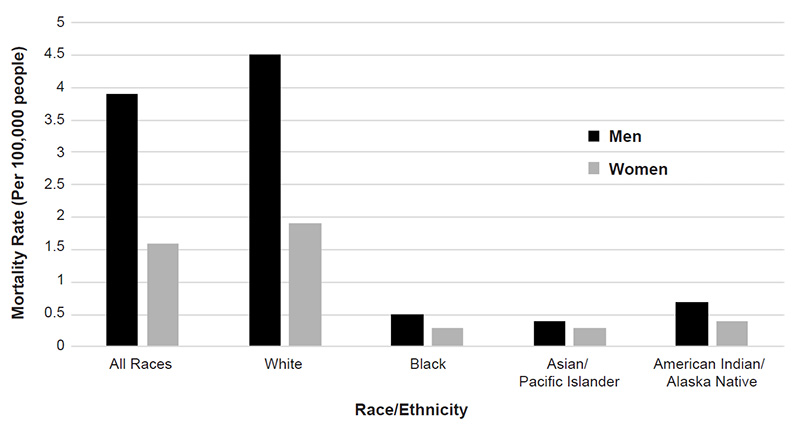
When detected and treated early, melanoma has a five-year survival rate of 98% [41]. Squamous cell carcinoma is associated with the greatest number of deaths attributed to nonmelanomas, and a 2013 study estimated that squamous cell carcinoma was responsible for 3,900 to 8,800 deaths in the United States in 2012 [42]. Previous estimates for annual nonmelanoma deaths have been closer to 2,000. As noted, of the three most common skin cancers, melanoma accounts for the most skin cancer-related deaths, and an estimated 7,650 people will die of the disease in 2022 [1]. Mortality rates associated with melanoma vary according to demographic factors; the rate is higher for men than for women (3.9 vs. 1.6 per 100,000), is highest for White men (4.5 per 100,000), and is lowest for Asian/Pacific Islander men and women (0.4 and 0.3 per 100,000, respectively) (Figure 4) [43].
Since the 1970s, the relative five-year survival rate for melanoma has increased significantly, from approximately 82% (1975–1977) to 94% (2018–2021), with a 10-year survival rate of greater than 92% [1,41,43]. However, this rate is lower among racial/ethnic minority populations; for example, the five-year survival rate rose from 57% to 68% for the Black population during the same time period [1,41,43]. This disparity in survival is primarily the result of melanoma being diagnosed at later stages in Black individuals [24,134].
UV radiation is a known carcinogen in humans [44]. Sources of UV radiation include the sun, as well as sunlamps, sunbeds, and other types of tanning devices. Exposure to UV radiation, predominantly sun exposure, has been the most significant factor associated with the three primary types of skin cancers. Approximately 90% of nonmelanomas and 65% of melanomas are associated with sun exposure [45].
In the United States, the incidence of basal cell carcinoma has increased in states with a higher UV index (an estimate of the amount of UV radiation reaching the surface of the earth), with a greater difference for squamous cell carcinoma [46]. The risk of melanoma, however, was not found to differ with variations in the UV index, with only a few of the states with the highest numbers of melanoma cases associated with higher rates of sun exposure year-round (Table 1) [1,46,47]. These findings may be explained by many factors, including exposure to the sun in other locations (e.g., during vacation), changes in residence, frequency of exposure, and genetic susceptibility to the effects of UV radiation [48]. The findings also point to the need for enhanced awareness and attention to sun protection regardless of the geographic location of residence.
Both the epidermis and the underlying dermis are susceptible to damage from UV exposure. UV-A rays penetrate to the dermis, where they alter structural and matrix proteins, leading to the aged appearance associated with chronic sun exposure. UV-B rays are readily absorbed in the outer epidermal layer and are the primary cause of sunburn. UV-B rays are more carcinogenic than UV-A rays, and UV-B rays are thought to act as tumor initiators, while UV-A rays act as tumor promoters [32]. UV radiation is known to damage the p53 tumor suppressor gene, which is often mutated at high frequency in skin cancers [49].
Exposure to UV rays from the sun has increased significantly over the past century, as the protection afforded by the atmosphere has decreased due to atmospheric ozone layer depletion [50]. Individuals born between 1960 and 1980 have experienced the greatest increases in lifetime UV dose because of ozone depletion. Cloud cover filters only 20% to 40% of remaining UV rays, glass blocks UV-B rays but only half of UV-A rays, and certain clothing provides little sun protection (e.g., a white t-shirt, particularly when wet, offers very little protection) [17,242]. Sunscreen provides a chemical or physical barrier to UV rays, but only when applied correctly and consistently [17].
Although UV exposure is the primary factor in the development of nonmelanomas, data are conflicting about the pattern of exposure (i.e., cumulative exposure versus intense, intermittent exposure). Exposure to UV radiation begins in early childhood, and 23% of lifetime exposure is reached by the age of 18 years (Table 2) [51,52]. The greatest accumulation occurs between the ages of 41 and 59 years, which would account for the increase in rates of skin cancers with advancing age [36,51].
The risk of basal cell carcinoma has been found to be higher with episodic acute overexposure to the sun (sunburn) than with a similar degree of continuous exposure [53,54]. In contrast, chronic (cumulative) exposure to the sun has been associated with a higher risk of squamous cell carcinoma [54,55]. The findings of a study of Asian individuals demonstrated that lifetime sun exposure was primarily associated with higher risk of squamous cell carcinoma among women, while early-age sun exposure was associated with a greater risk among men [56].
The pattern of exposure associated with melanoma has been debated, with some researchers finding a higher risk with episodic overexposure to the sun and other investigators finding a higher risk with chronic exposure [57,58,59,60,61,62]. One study found that the exposure pattern depends on the anatomic site; melanomas on the head and neck were associated with chronic exposure, and melanomas on the trunk were related to episodic exposure [63]. A meta-analysis of 57 studies published before 2002 supported a relationship between sunburn history and an increased risk for melanoma (relative risk: 2.03); the analysis also demonstrated an inverse relationship between continuous exposure and high risk [64]. Studies have shown that the risk of melanoma is doubled for an individual who had one blistering sunburn in childhood or adolescence or five or more sunburns at any age [6,65,66]. Additionally, a cohort study published in 2014 noted that individuals experiencing five or more blistering sunburns between 15 to 20 years of age have an 80% increased risk of developing melanoma and a 64% increased risk of developing non-melanoma skin cancer in their lifetimes [6,227].
Through widespread education and legislation regarding the dangers of indoor tanning, exposure to artificial UV radiation has decreased in recent years, but nearly 8 million adults still tan each year. Among adults, the rates of indoor tanning declined to 3.5% in 2015 [69]. The 2015 prevalence decreased to 5.2% among women and to1.6% among men [69]. The national Youth Risk Behavior Survey also indicates a continued decrease among adolescents, with 15.6% indicating that they used indoor tanning in 2009, compared with 7.3% in 2015 [67,68]. The highest rates of indoor tanning are among White women 18 to 21 years of age (20.4%). Among White adults who reported indoor tanning, 40.8% reported at least one sunburn in the past 12 months, compared with 33.9% of non-indoor tanners [69].
The high use of devices with known carcinogenicity has led to much research on the association between indoor tanning and skin cancers. More than 419,000 cases of skin cancer are diagnosed annually due to indoor tanning, including 245,000 basal cell carcinomas, 168,000 squamous cell carcinomas, and 6,200 melanomas [2]. Studies have shown an increased risk for basal cell (29%) and squamous cell carcinoma (83%) associated with use of a tanning device; people who first use a tanning device before 35 years of age have a 75% increased risk for developing melanoma [2,70]. The direct cost of medical care for indoor tanning-related skin cancers is approximately $350 million annually in the United States.
As of 2023, 20 states and the District of Columbia have passed legislation prohibiting indoor tanning for children younger than 18 years of age. In addition, 44 states have passed legislation to regulate indoor tanning among minors, including limiting exposure time, providing eye protection, and requiring parental consent [71]. The Society of Behavioral Medicine, the American Academy of Dermatology, and the American Academy of Pediatrics have all issued statements supporting the ban of indoor tanning for minors [224,225,226]. The World Health Organization and the U.S. Food and Drug Administration (FDA) have declared indoor tanning devices to be carcinogenic, and the Surgeon General issued a first-time warning on the dangers of UV radiation and indoor tanning in 2015 [2,72,73].
In addition to the risk factors already mentioned (age, sex, race/ethnicity, comorbid or previous conditions, and geographic location), other individual risk factors associated with the development of nonmelanoma skin cancers include physical characteristics that influence the response to UV rays, such as complexion and eye and hair color. A personal or family history of skin cancers also adds risk (Table 3) [9,32,33]. A low percentage of nonmelanomas are the result of industrial agents such as hydrocarbons, arsenic, coal tar, and ionizing radiation [9,32]. Exposure to UV rays is the most common risk factor for basal cell carcinoma across all racial/ethnic populations [28]. In the Black population, the most important risk factors for squamous cell carcinoma are chronic scarring processes (occurring in 20% to 40%) and areas of chronic inflammation [27,28].
RISK FACTORS FOR SKIN CANCER
| Type of Skin Cancer | Risk Factors | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Nonmelanomas |
| |||||||||||||||
| Melanomas |
| |||||||||||||||
| ||||||||||||||||
Basal cell carcinoma arises from the basal layer of keratinocytes in the epidermis. These lesions are most often localized and will gradually destroy healthy surrounding tissue if left untreated. Basal cell carcinoma is classified in histologic subtypes according to the degree of invasion, from superficial basal cell carcinoma to nodular, micronodular, and morpheaform (fibrosing or sclerosing) types. The most common form is a mixed type, followed by nodular, superficial, and micronodular [74]. The superficial and nodular subtypes generally follow a less aggressive clinical course than the other subtypes [33]. Basal cell carcinoma is slow growing and rarely metastasizes, with a rate of metastasis of 0.0028% to 0.55% [33].
Squamous cell carcinoma, which originates in keratinizing epidermal cells, differs from basal cell carcinoma because of its potential to grow rapidly and invade fatty tissues beneath the skin and to metastasize. The risk of metastasis for squamous cell carcinoma varies widely, with an average rate of 2% to 6% [7,75,76]. However, the rate of metastasis is 11% to 15% for lesions on the lip and is nearly 30% for tumors larger than 2 cm with poor cell differentiation [32]. Other risk factors associated with metastasis include increasing depth of invasion, location in old scars or areas of chronic radiation dermatitis, and the presence of a compromised immune system [32].
As many as 60% of squamous cell carcinomas evolve from actinic keratoses [77]. These premalignant growths develop as a result of epigenetic changes caused by chronic exposure to sunlight [76]. Actinic keratoses are slow growing, usually asymptomatic, and frequently resolve on their own, but may recur. If left untreated, actinic keratoses become malignant in 0.25% to 20% of cases [9]. Another precursor lesion is squamous cell carcinoma in situ (also called Bowen disease), in which malignant cells are confined to the epidermis [9,32].
Historically, squamous cell carcinomas have not been classified into subtypes; however, they exhibit a range of clinical behaviors from indolent to aggressive with significant metastatic potential. Researchers have recommended a risk-based classification system based on malignant potential, with categories of low (metastatic rate of 2% or less), intermediate (metastatic rate of 3% to 20%), high (metastatic rate of more than 10%), and indeterminate [78,228]. Examples of low-risk squamous cell carcinomas are those arising from actinic keratosis and those associated with HPV. Intermediate-risk subtypes include adenoid (acantholytic) squamous cell carcinoma and intraepidermal epithelioma with invasion. The high-risk subtypes include de novo squamous cell carcinoma, squamous cell carcinoma associated with predisposing factors (e.g., radiation, burn scars, immunosuppression), invasive Bowen disease, adenosquamous carcinoma, and malignant proliferating pilar tumors. Signet ring cell, follicular, papillary, and clear-cell squamous cell carcinomas are classified as indeterminate [78,228].
The early detection and diagnosis of skin cancers is crucial for selecting the appropriate treatment approach and to an optimum outcome. Early studies suggested that dermatologists were best at identifying skin cancers, but it is appropriate for primary care providers to conduct skin examinations and to evaluate suspicious lesions, especially given that 50% of all healthcare visits are to a primary care provider [79,80,81]. According to a survey of family physicians, as many as 74% of respondents said they treat skin cancers in their offices [82]. Identification of melanomas is essential for reducing their associated morbidity and mortality, as melanomas detected by primary care providers have a greater likelihood of being less invasive than those found by self-examination or examination by family members [81,83]. In general, referral to a dermatologist is appropriate for borderline or larger lesions, and review of pathology reports should include a dermatologist and/or surgical oncologist [75].
The primary challenges in diagnosing skin cancers are to distinguish between benign and malignant lesions and to identify lesions with malignant potential. The first steps in diagnosing skin cancers involve obtaining a history and physical examination and evaluating the clinical features of the lesion. Symptomatology does not play a large role in the detection and diagnosis of skin cancers, as early-stage lesions are usually asymptomatic. Preliminary diagnoses for nonmelanomas can be based on the clinical appearance of the lesion, but biopsy should be performed to determine a definitive diagnosis.
When evaluating a patient with a suspicious lesion, it is important to obtain a history of relevant risk factors and to perform a physical examination, with systematic inspection of the entire skin surface to determine the presence of other lesions. If squamous cell carcinoma is suspected, regional lymph nodes should be evaluated clinically and with imaging studies, when indicated [84]. Advanced lesions may be associated with nonhealing ulceration, bleeding, or pain [9,76]. A sore that does not heal may be a sign of either basal cell or squamous cell carcinoma.
The examination room should be brightly lit, and full-spectrum halogen light or combined incandescent and fluorescent light may be useful. A hand lens with a 7 to 10 times magnification is helpful for evaluating variation in pigment pattern, and dermoscopy has been shown to provide more accurate assessment of lesions than examination with the naked eye, resulting in fewer excisions of benign lesions [9,85,86,87,88]. In one study, instructing primary care physicians on how to use dermoscopy and the subsequent use of dermoscopy within the standard clinical examination significantly increased the sensitivity of referrals to dermatology specialists [89]. Photographs may be helpful for documenting changes in moles and dysplastic nevi over time.
Examination to identify skin cancers includes evaluation of such clinical characteristics as shape, elevation, nature of the surface, color, and type of border. When evaluating nonmelanomas, clinicians should consider differences in some clinical features among racial/ethnic populations to avoid incorrect diagnoses [28].
Basal Cell Carcinoma
The classic appearance of basal cell carcinoma is a pearly, waxy, or translucent papule or nodule with small telangiectatic vessels on its surface; this is the nodular type (Table 4) [7,8,9,32,33,76,90]. This type may occasionally appear similar to large pores or pits of the sebaceous skin of the central portion of the face (Image 3) [91]. Superficial and nodular basal cell carcinomas may look brown, blue, or black as a result of the presence of melanin. The morpheaform type usually presents as a whitish or yellowish, indurated scar-like plaque, often with indistinct borders [9,32,33].
CLINICAL FEATURES OF BASAL CELL CARCINOMAS
| Type of Basal Cell Carcinoma | Surface | Color | Border | Common Anatomic Sites | Similar in Appearance |
|---|---|---|---|---|---|
| Superficial | Scaly erythematous patch or plaque | Usually lacks pigment, but can be brown, blue, or black | Threadlike | Face, upper extremities, posterior trunk, lower extremities | Inflammatory skin disorder (psoriasis or nummular eczema) |
| Nodular | Pearly papule or nodule, frequently with small telangiectatic vessels | Brown, blue, or black | Rolled | Face, upper and lower extremities, neck, posterior trunk | Large pores or pits of sebaceous skin of central portion of face |
| Morpheaform (sclerosing) | Indurated scar-like plaque | Whitish or yellowish | Indistinct | Head and neck, trunk, arms and legs | — |

The most common sites for basal cell carcinomas are the head and neck (85% of cases) and the trunk [8,33]. The clinical features and most common anatomic sites of basal cell carcinoma are similar across all racial/ethnic populations. One difference is the prevalence of pigmentation in the lesion; pigmentation is present in more than half of basal cell carcinomas in individuals of color, compared with approximately 5% in the White population [28]. Among the Asian population, basal cell carcinomas often appear brown to glossy black and have a black, pearly appearance [28].
Squamous cell carcinoma usually presents as an ulcerated erythematous nodule, scaling patch, or superficial erosion on the skin or lower lip, but the clinical features of this nonmelanoma vary widely (Table 5) [7,9,32,33,76]. These lesions may also appear as a verrucous papule or plaque. Color also varies, and lesions may be reddish-brown, pink, or flesh-colored. Squamous cell carcinomas typically present as exophytic tumors, ranging in size from a few millimeters to centimeters. Larger lesions may appear crusted, erythematous, or eroded (Image 4). In contrast to basal cell carcinoma, overlying telangiectasias are uncommon. The margins may be ill-defined, and the lesion may be fixated to underlying structures [9,32].
CLINICAL FEATURES OF SQUAMOUS CELL CARCINOMAS
| Surface | Ulcerated erythematous nodule or superficial erosion; verrucous papule or plaque; larger lesions may appear crusted, erythematous, or eroded | ||
| Color | Reddish-brown, pink, or flesh-colored | ||
| Border | Ill-defined, may be fixed to underlying structures | ||
| Common Anatomic Sites | Head and neck (especially lip and ear), hands, forearms, upper trunk, lower legs | ||
| Similar in Appearance | Keratoacanthoma (usually dome-shaped papule with a central keratotic crater) | ||
| Premalignant Lesions |
|

Actinic keratosis (a premalignant form of squamous cell carcinoma) appears as small (size of a pinhead) rough spots that may reach several centimeters in diameter. They are typically pink-red or flesh-colored and feel rough to the touch. Changes such as pain, erythema, ulceration, induration, hyperkeratosis, and increasing size may suggest evolution of an actinic keratosis to squamous cell carcinoma. Some evolving lesions may become clinically indistinguishable from invasive squamous cell carcinoma during their development [92]. Squamous cell carcinoma in situ appears as a reddish patch that is usually larger than actinic keratoses, more scaly, and sometimes crusted.
Cutaneous squamous cell carcinoma may develop anywhere on the body but usually arises on sun-damaged skin. However, in individuals of color, the lesions develop primarily in areas of the body that are not exposed to the sun (such as the legs) [28]. Approximately 50% to 60% of squamous cell carcinomas occur on the head and neck (especially the lip and ear), and other common sites are the hands, forearms, upper trunk, and lower legs [7]. Actinic keratoses typically develop on the face, ears, back of the hands, and arms.
A biopsy should be performed on any suspicious lesion. Excisional biopsy is preferred for most cases [75,84,93]. A shave biopsy can be done for lesions that appear to be benign or for elevated, nodular lesions suggestive of basal cell or squamous cell carcinoma [75,76]. An incisional or punch biopsy may be considered for large lesions or when maximum preservation of tissue is desired (e.g., lesions on the palm or sole, a digit, the face, or an ear). An incisional biopsy should be performed through the thickest portion of the lesion and should include the vertical growth phase of the primary tumor, if present [9].
In cases of suspected squamous cell carcinoma, a core biopsy or fine-needle aspiration should be done on regional lymph nodes that are either palpable or appear abnormal on imaging studies [84].
Nonmelanoma skin cancers are staged according to the American Joint Committee on Cancer (AJCC) tumor, node, metastasis (TNM) classification [94]. Basal cell carcinomas are rarely staged due to limited risk of metastasis. However, because of the higher risk of metastasis of squamous cell carcinoma, staging criteria were provided in the seventh edition of the AJCC manual, published in 2009. The 2009 classification for cutaneous squamous cell skin carcinomas and a first-time separate classification for Merkel cell carcinoma provided a method of staging nonmelanoma skin cancers [94,229]. However, research showed that the tumor (T) classification for cutaneous squamous cell carcinoma failed to accurately stratify disease-related outcomes. As a result, the eighth edition of the AJCC TNM classification features a revised tumor classification that applies to only the head and neck of those with nonmelanoma skin cancers and includes the requirement to measure the maximum dimension (usually diameter) of every potential invasive cancer before assigning a T1–T3 category, which have also been updated depending on the size of the lesion. This has since been shown effective in the stratification of staging these diseases [229,230,231].
According to the 2017 AJCC system, early stage cutaneous squamous cell carcinoma is defined as no evidence of regional or distant metastasis, with stage I assigned to tumors 2 cm or less and stage II disease to tumors larger than 2 cm but smaller than 4 cm [94,230]. Stage III disease is defined by a tumor larger than 4 cm or by tumor extension into bone, perineural invasion or deep invasion (>6 cm beyond subcutaneous fat). Stage III may also be any size tumor in conjunction with clinical, histologic, or radiographic evidence of disease in one lymph node (3 cm or less) and no extranodal extension [94,230]. The characteristics of stage IV disease are direct or perineural tumor invasion of the skull base or axial skeleton, involvement of two or more lymph nodes, metastasis in one or more lymph nodes that is larger than 3 cm, or distant metastasis [94]. The regional lymph nodes, lung, and liver are the most common sites of metastasis [7].
The goals of treatment of nonmelanoma are cure, preservation of function, and cosmesis. Several treatment options are available, but surgery is the primary treatment modality, as it is the most effective and efficient way to achieve cure [84]. Among the surgical treatments are electrodessiccation and curettage, traditional surgical excision, and Mohs micrographic surgery; superficial therapies include cryotherapy, topical treatment with 5-fluorouracil or imiquimod, and photodynamic therapy (Table 6) [7,9,32,75,76,92,95,96,97,98,99]. Radiation therapy remains an adjunctive option or primary therapy, but it is associated with possible cosmetic damage and long-term sequelae, including secondary malignancies, non-healing ulcers (in up to 25% of lesions), decreased sensation, cataracts, and soft tissue, cartilage, bone, or brain necrosis [84].
TREATMENT OPTIONS FOR BASAL CELL AND SQUAMOUS CELL CARCINOMAS
| Treatment Option | Type of Tumors | Comments | 5-Year Cure Rate | ||
|---|---|---|---|---|---|
| Electrodesiccation and curettage | Low-risk tumors | A commonly used technique | >92% | ||
| Surgical excision | High-risk basal cell carcinoma, standard treatment for squamous cell carcinoma | A commonly used technique; offers good histologic control | >90% | ||
| Mohs micrographic surgery | Large, ill-defined tumors, hard-to-treat locations (head, neck, hands, feet), recurrent lesions | Offers best histologic control; saves greatest amount of healthy tissue; high cost | 95% to 99% | ||
| Radiation therapy | Lesions near eye, nose, ear | An option for patients who are not good candidates for surgery | >90% | ||
| Photodynamic therapy | Superficial basal cell carcinoma, large, extensive lesions, or multiple lesions | Excellent cosmetic outcome, with minimal damage to normal tissue | Not available | ||
| Topical fluorouracil (5-FU) | Superficial basal cell carcinoma, multiple lesions, difficult treatment sites | Nonvisible dermal involvement may persist; local skin reaction | Not available | ||
| Topical 5% imiquimod cream | Superficial basal cell carcinoma | Local skin reaction | Not available | ||
| Cryotherapy | Low-risk tumors | Specialized equipment and skills; long healing time | 92.5% | ||
| Laser surgery | Treatment secondary to failed topical medications | Risk of scarring and pigment loss greater than with other techniques | Not available | ||
| Hedgehog pathway inhibitors | Treatment of metastatic or locally advanced basal cell carcinoma | New class of treatment; long-term efficacy unknown. Should be considered in those not responding to surgery or radiation. | Not available | ||
| PD-1 inhibitors (checkpoint inhibitors) | Treatment of metastatic or locally advanced carcinomas |
| Not available |
Although basal cell carcinomas rarely metastasize, these lesions should be removed, as they can become large, destroying healthy surrounding tissue and causing disfigurement. Appropriate treatment is essential to minimize the risk of recurrence, which is important because recurrent basal cell carcinomas are usually more aggressive than primary lesions of this type [32,232].
The American Academy of Dermatology recommends standard excision with a 4-mm margin of uninvolved skin around the tumor and/or biopsy site to a depth of the mid-subcutaneous adipose tissue with histologic margin assessment for low-risk primary basal cell carcinoma. For high-risk Basal cell carcinoma, the recommended approach is Mohs microsurgery.
(https://www.jaad.org/article/S0190-9622(17)32529-X/fulltext Last Accessed: February 21, 2025)Strength of Recommendation/Level of Evidence: A1 (Recommendation based on consistent and good-quality patient-oriented evidence measuring outcomes that matter to patients: morbidity, mortality, symptom improvement, cost reduction, and quality of life)
A systematic review of the literature has shown that surgery or radiation therapy is the most effective treatment for basal cell carcinomas, with surgery associated with the lowest rates of failure [102,232]. Guidelines developed by the National Comprehensive Cancer Network (NCCN) recommend electrodessication and curettage for low-risk lesions, defined as lesions less than 1.5 cm in diameter and of less aggressive subtypes, as well as lesions in more favorable locations [103]. However, the technique cannot be used in a hair-bearing area, as tumor that extends into follicular structures may not be adequately removed [103]. Traditional surgical excision, superficial therapies (where radiation and surgery are contraindicated), and radiation therapy (typically reserved for those older than 60 years of age) are other options [103].
Surgical excision is the recommended treatment for high-risk basal cell carcinomas, and Mohs micrographic surgery and radiation therapy are other options [103]. In all cases of surgical excision, the margins should be evaluated postoperatively; Mohs micrographic surgery or repeat excision should be done if the margins are positive. Mohs surgery is also the treatment of choice for most morpheaform (sclerosing) basal cell carcinomas, as well as for recurrent lesions, tumors in high-risk locations, lesions that are large and ill-defined, or in instances when maximal tissue conservation is critical [9,75,76].
The high cost of Mohs micrographic surgery has raised concern about whether the cost is warranted. A review of the literature involving comparisons of Mohs surgery and surgical excision demonstrated that Mohs surgery was associated with the highest initial cure rates and the lowest recurrence rates [104]. In addition, Mohs surgery was found to be cost-effective, primarily because traditional surgical excision was associated with higher costs for frozen sections, ambulatory facility costs, and the cost of repeat excision [104].
Although a surgical approach is used most often for basal cell carcinomas, radiation therapy can also be effective. This modality is helpful for patients who are not considered to be good candidates for surgery, and it is useful for lesions near the eye, nose, or ear. However, long-term cosmesis is less favorable. Radiation therapy can also be used as an adjunct to surgery for high-risk tumors. Due to the long-term risks associated with exposure to radiation, this approach should be avoided in patients younger than 60 years of age [75]. Radiation is also contraindicated in patients with genetic predisposition to skin cancer and should likely be avoided in patients with connective tissue diseases [103].
In 2006, a National Institutes of Health Consensus Statement indicated that photodynamic therapy with 5-aminolevulinic acid (ALA) is a safe and effective method for treating superficial basal cell carcinoma [98]. The following year, the International Society for Photodynamic Therapy in Dermatology published evidence-based recommendations on the use of photodynamic therapy with ALA or methyl aminolevulinate (MAL) [99]. The authors of these recommendations concluded that photodynamic therapy was effective and reliable for superficial basal cell carcinoma, offering excellent cosmetic outcomes, and was beneficial for the treatment of large, extensive, and multiple lesions [99]. In addition, five-year follow-up demonstrated long-term efficacy of photodynamic therapy with MAL for the treatment of superficial or nodular basal cell carcinoma [99]. A synthesis of international guidelines for the use of photodynamic therapy published in 2019 also supported the use for superficial and certain thin nodular basal cell carcinomas [233].
Treatment with topical 5-fluorouracil can be used for superficial basal cell carcinomas, and intralesional chemotherapy (5-fluorouracil and interferon) has been found to be effective for patients with numerous lesions [9,76,222]. Topical treatment with an immunomodulator has shown encouraging results for the treatment of superficial and nodular basal cell carcinomas.
Cryotherapy with liquid nitrogen or nitrous oxide can be used for low-risk tumors, but the approach calls for specialized equipment and skills, and several weeks may be needed for complete healing [9,75]. The long-term efficacy of laser surgery for the treatment of infiltrative or recurrent lesions is not known. Although this modality has some advantages, its use is limited by safety hazards and inconvenience [75].
Due to advances in the understanding of pathogenesis of basal cell carcinoma, a newer class of drugs—hedgehog pathway inhibitors—was first approved by the FDA in 2012 for the treatment of metastatic or locally advanced basal cell carcinoma [103,154,234]. Hedgehog pathway inhibitors work by selectively blocking Smoothened (Smo), a key transmembrane protein involved in hedgehog signal transduction of cancerous epithelial cells [101,154]. The 2025 NCCN practice guidelines recommend consideration of a hedgehog pathway inhibitor in patients who have exhausted other surgical and radiation treatment options. It has also been found that this class of drugs may be effective in the treatment of cutaneous squamous cell cancer of the head and neck, although this use is off-label [103,154,234]. More studies are needed to determine the efficacy and long-term outcomes of this novel treatment modality; however, in one trial, 65% of patients with locally advanced disease and previously treated with standard therapies showed significant improvement while 11% significantly worsened.
As with basal cell carcinomas, treatment of squamous cell carcinoma depends on a variety of factors, including tumor characteristics (i.e., size, location, and degree of histologic differentiation) and patient characteristics (e.g., age, physical condition). In general, curettage and electrodessication is recommended for localized, low-risk lesions, with surgical excision and radiation therapy as additional options. Localized, high-risk lesions (larger than 2 cm in diameter on the trunk or extremities or larger than 1 cm on the face or neck) should be treated with surgical excision or Mohs micrographic surgery [84]. Mohs micrographic surgery is preferred when the amount of tissue removed must be kept to a minimum for cosmetic reasons or to maximize function [7]. The NCCN recommends 4- to 6-mm clinical margins when excising squamous cell carcinomas [84]. The risks of radiotherapy may outweigh the benefits, particularly for younger patients. It should be noted that the use of radiation alone for nodal metastasis is not recommended, due to poor control and survival, and clinical trial data regarding the use of adjunctive radiation therapy for regional disease are inconclusive [84].
As with basal cell carcinomas, radiation therapy may be used for patients who are not surgical candidates, when it is critical to preserve function or cosmesis, or as an adjunct to surgery for high-risk tumors, and should not be routinely used for patients younger than 60 years of age [84].
Although photodynamic therapy has been effective for superficial squamous cell carcinoma in some small studies, the recurrence rate has been as high as 69% (mean: 24%), and complete response rates to treatment are estimated to be between 48% to 89% [84,105,106]. Thus, photodynamic therapy was not recommended for the treatment of squamous cell carcinoma in the International Society for Photodynamic Therapy in Dermatology guidelines [99].
Superficial therapies may yield lower cure rates than surgery and, as such, should be used only for shallow squamous cell cancers or for individuals in whom surgery or radiation is contraindicated or impractical [84].
Cryotherapy is a common approach for actinic keratosis [84]. Other treatment options for these premalignant lesions are photodynamic therapy; ablative skin resurfacing; chemical peels; topical treatment with 5-fluorouracil or imiquimod; and systemic treatment with retinoids or capecitabinem [84,92,98].
Palpable regional lymph nodes should be surgically evaluated, and lymph node dissection should be done when the findings are positive on evaluation of samples from open biopsy or fine-needle aspiration [84]. Radiation therapy should be used for individuals who have palpable lymph nodes in the head and neck region. For individuals with palpable nodes in the trunk or extremities, radiation therapy should be considered after node dissection [84].
As noted, appropriate treatment of basal cell and squamous cell carcinomas can lead to high cure rates. However, a second nonmelanoma will develop in approximately 60% of individuals within 10 years after treatment of a first skin cancer, and the risk for cutaneous melanoma is also increased [107,108,109]. An estimated 30% to 50% of patients will develop a recurrent cutaneous squamous cell carcinoma within five years after treatment (70% to 80% of these recurrences develop within two years) [84,110]. A primary risk factor for recurrence of either basal cell or squamous cell carcinomas is size, in accordance to location, as follows [84,103]:
20 mm or more: Trunk, extremities
10 mm or more: Cheeks, forehead, scalp, neck
Any, not dependent on size: So-called mask areas of the face
Poorly defined borders, immunosuppression, and site of previous radiation therapy are other risk factors for recurrence of both types of nonmelanomas; site of chronic inflammatory process, neurologic symptoms, rapid tumor growth, moderate or poor differentiation, and thickness increase the risk of recurrent squamous cell carcinomas [84].
The NCCN recommends a history and physical examination, including a complete skin examination, every 6 to 12 months for 2 years after treatment and then, if appropriate, a reduced follow-up schedule for basal cell carcinoma; follow-up after treatment for squamous cell carcinoma is based on the extent of disease (Table 7) [84,103]. Follow-up for all patients should include extensive education on sun protection and self-examination [84,103].
NATIONAL COMPREHENSIVE CANCER NETWORK RECOMMENDATIONS FOR FOLLOW-UP AFTER TREATMENT FOR NONMELANOMAS
| Disease | Follow-Up | Frequency | ||
|---|---|---|---|---|
| Basal cell carcinoma |
| Every 6 to 12 months for 5 years, then assess risk and adjust follow-up frequency thereafter | ||
| Squamous cell carcinoma, localized |
| Every 3 to 12 months for 2 years, then every 6 to 12 months for 3 years, and annually thereafter | ||
| Squamous cell carcinoma, regional |
| Every 2 to 3 months for 1 year, then every 2 to 4 months for 1 year, then every 4 to 6 months for 3 years, and every 6 to 12 months annually thereafter |
The factors associated with an increased risk of melanoma, in decreasing order of importance, include [100,235]:
A persistently changed or changing mole
Adulthood (compared with childhood)
Irregular varieties of pigmented lesions, including dysplastic nevi and lentigo maligna
A congenital mole
White race
A personal or family history of melanoma
Immunosuppression
Sun sensitivity
Excessive sun exposure
A review of data on nearly 363,000 individuals who were screened for melanoma demonstrated five factors that independently increased the likelihood of melanoma: history of previous melanoma, age older than 50 years, lack of a regular dermatologist, presence of a changing mole, and male sex [111,235].
A model has been developed by the National Cancer Institute (NCI) to calculate the absolute risk of melanoma based on risk factors that are easily determined during a routine history and physical examination. The model is available online at https://mrisktool.cancer.gov.
Melanomas originate from melanocytes, epidermal dendritic cells that synthesize melanin. Undetected primary melanomas undergo two growth phases: the radial growth phase and the vertical growth phase. In the first phase, the tumor cells are confined to the epidermis or are locally invasive without evidence of potential for growth or metastasis. In the latter stage, melanoma cells expand into the dermis and subcutaneous tissue and are at risk for systemic metastasis [112].
Research has shown that melanomas develop at different anatomic sites through divergent pathways [113,114]. For example, the number of moles has been most strongly associated with melanoma of the trunk, whereas severe, painful sunburn (intense, episodic exposure) has been most strongly related to melanoma on an upper extremity [113]. The molecular basis of melanoma continues to be explored, and mutations in several oncogenes have been linked to melanoma. Many researchers believe that the development of melanoma is a complex interaction among genetic, environmental, and possibly other factors [115,235].
Several studies have been conducted on the relationship between atypical moles (dysplastic nevi) and the risk of melanoma. Most people have several moles (10 to 40), but melanoma is less likely to arise from these typical moles than from dysplastic nevi [116]. Approximately 10% of people have at least one dysplastic nevus, which is generally larger than a typical mole and has irregular or indistinct borders [116]. The development of dysplastic nevi tends to occur in families, and often, several members of a family have a large number of dysplastic nevi; the risk of melanoma is higher for these individuals than for the general population. Researchers have found that the occurrence of melanoma is 10 times greater for individuals with five or more dysplastic nevi compared to those without, and the risk of melanoma increases as the number of dysplastic nevi increases [32,116,117,118]. The lifetime risk of melanoma is more than 50% for individuals who have both dysplastic nevi and a family history of melanoma [9].
Melanomas are categorized into four main histologic subtypes: superficial spreading, nodular, lentigo maligna, and acral lentiginous. Superficial spreading melanoma is the most common subtype, accounting for 70% of all melanomas [7,32]. Nodular melanoma accounts for 10% to 15% of all melanomas, lentigo maligna for 4% to 15%, and acral lentiginous for 2% to 8% [23,32,236]. The frequency of these subtypes varies according to ethnicity, with superficial spreading melanoma occurring most frequently in the White and Hispanic populations, and acral lentiginous melanomas appearing more often in Black and Asian/Pacific Islander populations than in the White population [27,28,32].
There are also differences in the prevalence of these subtypes with respect to the age of the patient and the anatomic location of the lesion. For superficial spreading melanoma, the mean age at the time of diagnosis is 59 years and the most common anatomic sites are areas of intermittent sun exposure, including the trunk (especially in men), the legs (especially in women), and the back (in both) [119,236]. In contrast, lentigo maligna occurs most often in individuals who are 70 to 80 years of age and typically develops in chronically sun-damaged areas (e.g., the face, neck, back of hands) [32]. Lentigo maligna may be difficult to diagnose if it develops in areas of sun-damaged skin [120]. Acral lentiginous melanoma appears on the palmar and plantar surfaces, the digits, and subungual areas [25].
Most melanomas are detected by nonphysicians; one study found that 72% of melanomas were found by the individual or his or her family or friend [121]. Although this finding points to the importance of self-examination, the role of healthcare providers cannot be overstated, as they have typically detected thinner melanomas than those found by nonphysicians, and this earlier detection increases the likelihood of cure [122]. For example, in another study, 53% of melanomas were self-detected, but the incidental rate of melanoma detected by dermatologists was 80% [237]. Healthcare providers can also detect melanomas in anatomic areas that are outside an individual's view [122].
The history, physical examination, and biopsy are integral to diagnosing melanoma. Evaluating the clinical and pathologic features to determine the stage of disease is essential for selecting appropriate treatment.
As with squamous cell carcinomas, the clinical features of melanomas vary according to subtype (Table 8) [7,9,32,33,76]. Detection and diagnosis rely on careful evaluation of the appearance and anatomic site of the lesion and signs and symptoms of metastasis.
CLINICAL FEATURES OF MELANOMAS
| Type of Melanoma | Surface | Color | Border | Common Anatomic Sites | Similar in Appearance | Premalignant Lesions |
|---|---|---|---|---|---|---|
| Superficial spreading | Flat or slightly raised | Dark with variegated colors. Variation in pigment pattern, color (occasionally amelanotic). | Irregular, sometimes notched | Back (men); back and lower legs (women) | — | Dysplastic nevi (papular lesions, up to 6 mm or larger; cobblestone surface with variable mixture of tan, brown, and red or pink coloration; characteristically hazy and indistinct borders) |
| Nodular | Dome-shaped or pedunculated | Black, brown, blue, gray, tan, red. Variation in pigment pattern, color (occasionally amelanotic). | Smooth or regular | Back (men); back and lower legs (women) | Blood blisters, hemangiomas, nevi, or polyps | |
| Lentigo maligna | Flat, focal papular or nodular areas | Dark brown, reddish-brown, blue-black. Variation in pigment pattern, color (occasionally amelanotic). | Scalloped and convoluted | Sun-damaged, sun-exposed sites (face, neck, back of hands) | — | |
| Acral lentiginous | Flat or nodular | Brown, black, multicolored. Variation in pigment pattern, color (occasionally amelanotic). | Irregular, sometimes notched | Palms, soles, nail beds, mucous membranes | — |
Appearance
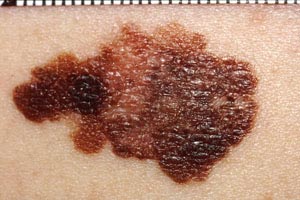
With melanomas, the most important feature is a change in appearance over time. As the lesion develops by penetrating deeper into the skin, the borders become irregular and may be notched (Image 5). The color and pigment pattern vary. Occasionally, melanomas are amelanotic and may be lighter than the surrounding skin or may be red. An increase in size or a change in color is noted by the patient in approximately 70% of early lesions [123]. Subungual melanomas are usually characterized by a pigmented band on the nail (typically more than 3 mm wide), variable pigment, a rapid increase in size, and the presence of a solitary lesion [27]. Bleeding, ulceration, and pain may be present in advanced disease.
As with nonmelanomas, detection focuses on distinguishing melanoma from nonmelanoma. In 1985, the ABCD rule was developed to help physicians distinguish melanomas from benign lesions (Table 9) [124]. According to this system, A represents asymmetry; B, border irregularity; C, color; and D, diameter (Image 6, Image 7, Image 8, and Image 9). "E" (evolving) was added to the rule to recognize the importance of changes in the size, shape, surface, shades of color, or symptoms (e.g., itching, tenderness), and it is considered the most important factor in diagnosing melanoma [125]. This system has a sensitivity of about 65% to 80%, primarily because some melanomas may be smaller than 6 mm, some may have a regular shape, and some may lack color variation [126].
ABCDE RULE FOR DISTINGUISHING BENIGN TUMORS FROM MELANOMAS
| Criteria | Benign Tumors | Melanoma |
|---|---|---|
| A: Asymmetry | Symmetric | Asymmetric |
| B: Border | Clear-cut, distinct border | Irregular border |
| C: Color | Uniform light or dark pigment | Pigment variegation |
| D: Diameter | <6 mm (usually) | ≥6 mm |
| E: Evolving | No change over time | Change in size, shape, surface, shades of color, or symptoms |



Dysplastic nevi, common precursors to melanoma, appear as macular or papular lesions, and they may be present in great numbers. They may be as large as 6 mm and have a cobblestone surface with hazy or indistinct borders (Image 10). The pigment pattern is highly varied; colors can include a mixture of tan, brown, and red or pink.

Anatomic Sites
In general, melanomas primarily occur in sun-exposed areas in White and Hispanic individuals and in sun-protected areas in Black, American Indian/Alaska Native, and Asian/Pacific Islander populations [2,27,28,127]. Specific anatomic sites vary among racial/ethnic groups. Among White and Hispanic individuals, the head, neck, and trunk are the most common sites for melanoma in men, and the lower part of the leg (knee to ankle) and the head and neck are the most common sites for women [113]. The trunk is the primary site for American Indian/Alaska Native individuals; the lower extremity is a common site for Hispanic, Black, and Asian/Pacific Islander individuals [2,127]. The foot is a common site for Black and Asian/Pacific Islander individuals, and mucosal and subungual sites are also common in these populations [2,127,128,129]. Uveal melanomas are rare but are the most common intraocular malignant lesions in adults [130].
Signs and Symptoms of Metastasis
Information from the history and physical examination can help in determining whether the melanoma has metastasized. Signs and symptoms such as general malaise, weight loss, headaches, visual difficulty, or bone pain are indicative of metastasis. If metastasis is suspected, imaging of the liver, lung, bone, and brain should be done, as these are the most common sites of metastasis [94].
When melanoma is suspected, full-thickness excision should be done when possible [25,76]. An excisional biopsy allows for the determination of the thickness of the melanoma, an important clinical and prognostic factor [131,132].
A full-thickness incisional biopsy or punch biopsy can be done on very large lesions or lesions in such anatomic areas as the palm or sole, a digit, the face, or an ear; in these cases, the biopsy should be done through the clinically thickest portion of the lesion [132]. A shave biopsy should be done only when the suspicion of melanoma is low, as this type of biopsy may compromise pathologic assessment [132]. All biopsy specimens should be evaluated by a pathologist experienced in pigmented lesions [132].
As with nonmelanomas, melanoma is staged according to the AJCC TNM classification (Table 10) [94]. Two primary factors considered in staging the melanoma are thickness (Breslow thickness) and ulceration [94]. In 2017, the AJCC TNM classification was updated and the requirement of mitotic rate for defining T1 tumors was removed, the Breslow stratification was lowered to 0.8 mm, and new staging subdivisions were added [94,231].
AMERICAN JOINT COMMISSION ON CANCER TNM CLASSIFICATION FOR MELANOMA
| Tumor (T) | |||||
| Tis | Melanoma in situ | ||||
| T1 | ≤1.0 mm |
| |||
| T2 | 1.0–2.0 mm |
| |||
| T3 | 2.0–4.0 mm |
| |||
| T4 | >4.0 mm |
| |||
| Regional Lymph Nodes (N) | |||||
| N0 | No regional metastases detected | ||||
| N1 | 1 lymph node |
| |||
| N2 | 2 or 3 lymph nodes |
| |||
| N3 | 4 or more metastatic lymph nodes, matted lymph nodes, or combinations of in-transit metastasis/satellite(s) and metastatic lymph nodes |
| |||
| Metastasis (M) | |||||
| M0 | No detectable evidence of distant metastasis | Normal LDH | |||
| M1a | Distant skin, subcutaneous, or lymph node metastasis |
| |||
| M1b | Lung metastasis with or without M1a sites of disease |
| |||
| M1c | Distant metastasis to non-CNS visceral sites with or without M1a or M1b sites of disease |
| |||
| M1d | Distant metastasis to CNS with or without M1a, M1b, or M1c sites of disease |
| |||
Tumor thickness is the most important prognostic factor for early stage melanoma, with highly significant decreases in 5-year and 10-year survival as thickness increases [32,94,133]. Ulceration is the next most important prognostic factor. The Clark level of invasion is no longer used in staging melanoma; this factor had been used in staging melanomas since 1969, but other factors have now been found to be more strongly correlated with survival rates [94].
Staging of regional lymph nodes is determined primarily by the number of involved nodes and tumor burden (micrometastasis or macrometastasis). Overall, the disease status of the lymph nodes is the most important prognostic factor for melanoma [94,135]. The M classification is defined by the site of metastasis and the serum lactate dehydrogenase (LDH) level [94]. Although it is uncommon to include a laboratory value in a staging system, the serum LDH level has been found to be a highly significant predictor of outcome for patients who have advanced stage disease [94].
After the TNM factors have been determined, a melanoma is assigned a stage based on defined groupings, from stage 0 (melanoma in situ) to stage IV (distant metastasis) [94]. Stage I melanoma is localized (no involved lymph nodes) and is subcategorized as stage IA (0.8 mm thick or less with or without ulceration (T1a) or 0.8–1.0 mm with or without ulceration (T1b) or stage IB (1.0–2.0 mm thick without ulceration).
Stage II melanoma is also localized; stage IIA lesions are 1–2.0 mm thick with ulceration or 2.0–4.0 mm thick with no ulceration; stage IIB lesions are 2.0–4.0 mm thick with ulceration or more than 4.0 mm thick with no ulceration; stage IIC lesions are more than 4.0 mm thick with ulceration [94].
Regional lymph nodes are involved with stage III melanoma. When lymph nodes are evaluated clinically only, there are no subclassifications of stage III disease. However, when lymph nodes are evaluated pathologically, this stage is subclassified into [94]:
Stage IIIA: T1a/b–T2a with one to three clinically occult nodes
Stage IIIB:
T1a/b–T2a with one to three nodes clinically detected or one node with in-transit metastasis/satellite(s) without regional lymph node disease; or
T2b–T3a with clinically occult or clinically detected in one to three nodes or one node with in-transit metastasis/satellite(s) without regional lymph node disease
Stage IIIC:
T1a–T3a with at least one lymph node clinically occult or clinically detected or in-transit metastasis/satellite(s) and/or presence of any matted nodes in two or more nodes, or
T3b/T4a with any lymph node involvement, or
T4b with one to three lymph nodes clinically occult or clinically detected, with or without in-transit metastasis/satellite(s), or
T0 with at least two nodes involved and one node clinically detected or at least one node with in-transit metastasis/satellite(s) with clinically or occult or clinically detected
Sentinel lymph node biopsy is considered by many to be a standard-of-care procedure for obtaining information on involvement of lymph nodes for staging melanoma, although fine-needle aspiration or core biopsy is also used [136,137]. The AJCC Cancer Staging Manual notes that if either of these methods are performed in the absence of complete nodal dissection, the N category of the TNM classification should be noted with a suffix of (sn) for sentinel node biopsy or (fn) for fine-needle aspiration or core biopsy [94].
Approximately 84% of individuals with melanoma have localized disease at the time of diagnosis [132]. Regional disease is present at the time of diagnosis in approximately 9% of individuals and distant metastasis in approximately 4% [132]. However, these rates vary significantly across racial/ethnic populations, with much higher rates of more advanced disease among minority populations and lower five-year survival rates [1,47,204]. In a study of 1,690 melanoma cases in Miami-Dade County (Florida), melanoma was diagnosed at later stages in Black and Hispanic populations than in White populations. Regional disease was evident at the time of diagnosis in 21% of Black individuals, compared with 11% of Hispanic individuals and 7% of White individuals; the corresponding rates for distant disease were 31%, 16%, and 9% [24]. Other studies have confirmed these disparities [127,204]. In addition, the rate of thinner melanomas was reported to be lower among Asian/Pacific Islander individuals than among White individuals (49% vs. 66%) [127].
The goal of treatment of newly diagnosed melanoma is to remove all malignant tissue and to minimize the risk of local recurrence. Melanomas in children should be treated as aggressively as those in adults [138]. Surgical excision should be done for all local and regional disease, with adequate clinical margins. A systematic review published in 2016 indicated that for melanomas less than 2 mm, a 1-cm margin appears to be wide enough, and for melanomas greater than 2 mm, a 2-cm margin is recommended [238]. However, there is still much debate and insufficient evidence on the optimal excision margins for melanoma. It is unclear if a margin wider than 2 cm would result in better outcomes [139,238]. In its guidelines for care of primary cutaneous melanoma, the American Academy of Dermatology and the NCCN recommend margins according to the thickness of the lesion (Table 11) [93,132].
Historically, the literature has shown no benefit to adjuvant therapy for stage II or III melanoma, but this has changed due to new clinical trial data [140]. In 2021, the FDA approved pembrolizumab for adjuvant treatment of Stage IIB or IIC (i.e., high-risk) melanoma following the completion of a phase III clinical trial to assess the safety and efficacy in preventing disease recurrence in adults and adolescents [244]. The NCCN advises that adjuvant treatment with pembrolizumab for Stage IIB and IIC melanomas can actively reduce relapse events, even though the effect on overall survival is currently unknown; the clinical trial cited in the FDA approval will run until 2033 to help determine this [132,245]. Accurate pathologic staging is critical to guide decision-making, and the benefits of pembrolizumab adjuvant therapy should be discussed with patients and weighed against the potential for significant systemic toxicity (e.g., thyroid, kidney, liver).
Interferon alfa-2b has provided some benefit for patients with stage III disease, including significant improvement in recurrence-and disease-free survival and in overall survival, although results of a 20-year study published in 2016 show no improvement or benefit in patients with minimal stage III melanoma, defined as melanoma in only one lymph node [141,142,143,239]. Interferon is associated with severe toxicity in almost half of patients treated with the high-dose protocol approved by the FDA. Factors to consider are the goal of treatment, the quality of life, and the cost [144,145]. Studies are focusing on ways to optimize immunotherapy and on gaining a better understanding of melanoma biology and tumor immunology [141,146,147,239].
Hyperthermic isolated limb perfusion is an option for patients with stage III unresectable in-transit metastasis [132]. This approach involves melphalan and tumor necrosis factor (TNF), and some studies have indicated a high response rate; however, the NCCN notes that TNF-alpha is currently unavailable in the United States [148]. Locoregional radiation therapy is another option for stages IB and higher; enrollment in a clinical trial of neoadjuvant therapy should also be considered for stages II and higher [132]. The NCCN recommends nivolumab for stage IIIB/C patients only.
Metastatic melanoma (stage IV) can be cured in certain patients depending primarily on the site(s) of metastases [132] The prognosis for patients with distant disease has significantly improved due to the development of effective systemic therapies [132]. If disease is limited (resectable), surgical resection is the preferred option, and nivolumab, pembrolizumab, or high-dose ipilimumab may be used after excision [132]. Immunotherapy with either interferon alfa-2b or interleukin-2 (IL-2) has led to response rates of 10% to 20% in appropriately selected patients, and complete responses achieved with immunotherapy seem to be more durable than those obtained with chemotherapy [148]. However, the toxicity associated with immunotherapy can be severe. Cytotoxic therapy may be considered on a case-by-case basis but is typically not preferred [132].
The NCCN recommendations for first-line treatment of metastatic melanoma or unrescectable disease include checkpoint immunotherapy (anti-PD-1 monotherapy with pembrolizumab or nivolumab or nivolumab/ipilimumab); for BRAF-mutated disease, the recommendation is for BRAF-targeted therapy (BRAF/MEK inhibitor combination therapy with dabrafenib/trametinib, vemurafenib/cobimetinib, or encorafenib/binimetinib) [132]. Other first-line recommendations include pembrolizumab/low-dose ipilimumab and, for BRAF-mutated disease, combination targeted therapy (vemurafenib/cobimetinib) plus immunotherapy (atezolizumab). Enrollment in a clinical trial should be discussed with patients with stage IV melanoma [132]. Systemic chemotherapy is preferred for disseminated (unresectable) disease. Palliative resection or radiation therapy should be considered for individuals with brain metastases [132]. Systemic therapy is also an option for these individuals [132].
Since 2011, the FDA has approved several new treatment options for melanoma, including ipilimumab, a chemotherapeutic agent for adjuvant treatment of stage III melanoma and the treatment of nonresectable or metastatic melanoma [152]. In clinical trials, ipilimumab improved survival rates in patients with advanced disease compared to the use of tumor vaccine [152,153]. It is the first in the monoclonal antibody group of medications to target an antigen (CTLA-4) on the surface of T cells. The approved dosage for unresectable or metastatic melanoma is 3 mg/kg administered intravenously every three weeks for four doses [154]. The most common side effects are fatigue, diarrhea, pruritus, and rash. The NCCN no longer recommends ipilimumab monotherapy for stage III patients because combination nivolumab/ipilimumab has been shown to improve outcomes in comparison [132]. Patients with stage IV disease with previous exposure to anti-PD-1 agents may benefit from ipilimumab monotherapy.
Vemurafenib is a BRAF kinase inhibitor and is approved for the treatment of advanced melanoma in patients with the BRAFV600E mutation, as detected by an FDA-approved test [155]. A clinical trial involving 675 patients with previously untreated, metastatic melanoma with this mutation found that overall survival was significantly better with vemurafenib (84%) than with dacarbazine (64%) [156]. Compared with dacarbazine, vemurafenib was associated with a 74% reduction in the risk of either death or disease progression. The recommended dose is 960 mg twice daily orally, until disease progression or unacceptable toxicity [154]. In cases of intolerable toxicity, the treatment should be interrupted and then restarted at a lesser dose (not less than 480 mg twice daily). In 2015, cobimetinib was approved for use in combination with vemurafenib in patients with BRAF-mutated metastatic or unresectable melanoma [247]. In 2020, the FDA approved a new combination therapy for unresectable or metastatic BRAF-mutated melanomas, vemurafenib/cobimetinib plus atezolizumab [243]. Atezolizumab is an IV infusion given every two weeks, until disease progression or unacceptable toxicity and is associated with greater progression-free survival [154].
In 2013 and 2014, three additional drugs (dabrafenib, trametinib, and pembrolizumab) were approved for the treatment of patients with advanced or unresectable melanoma who are not responding to other medications [157]. These agents have different mechanisms of action and therefore present new options for patients with refractory melanoma. Pembrolizumab, the first anti-PD-1 drug (a monoclonal antibody) approved by the FDA, inhibits negative immune regulation [154,157]. In 2017, nivolumab, also a PD-1 blocker, gained FDA approval for adjuvant treatment of cutaneous melanoma; nivolumab monotherapy was found to be at least as effective as ipilimumab monotherapy, with fewer adverse effects [132,246]. In 2018, the FDA approved two new combination drugs for the treatment of patients with unresectable or metastatic melanoma with a BRAFV600E or BRAFV600K mutation as detected by an FDA-approved test: trametinib/dabrafenib and encorafenib/binimetinib [150,151].
At one time, lymph node dissection was done routinely with excision, because of the significant association between the disease status of the nodes and survival. However, the rate of metastasis to regional nodes is low for early stage melanoma; nodes are involved in approximately 1% of melanomas that are 0.75 mm or less thick, in approximately 15% of melanomas that are 1.0–2.0 mm thick, and in approximately 15% to 20% of lesions of so-called intermediate thickness (1.2–3.5 mm) [159,160,161]. To avoid the morbidity associated with potentially unnecessary lymph node dissection, the procedure is no longer done routinely and its indications have been debated.
The most definitive trial to date on the role of sentinel lymph node biopsy is the Multicenter Selective Lymphadenectomy Trial I (MSLT-I), in which 1,269 patients with melanomas of intermediate thickness were randomly assigned to either excision with sentinel node biopsy and lymph node dissection if metastasis was found or to excision and observation, with dissection done only when disease became clinically evident in a node [161]. Several important findings of the study have been noted [136,137,161]:
Presence of metastases in the sentinel node was the most important prognostic factor, with a five-year survival rate of 90% for patients with no metastasis in the sentinel node and 72% for patients with metastasis in the sentinel node.
The five-year survival rate was significantly higher for patients who had immediate dissection after sentinel node biopsy compared with patients who had delayed dissection (72% vs. 52%), although five- year melanoma-specific survival rates were similar (approximately 87%).
The similarity in the incidence of node metastases in patients who had excision and observation and the total incidence of metastasis detected by sentinel node biopsy suggests that micrometastatic disease will become clinically detectable disease if the node is not removed.
Sentinel node biopsy detected micro-metastases a median of 16 months earlier than metastasis can be detected in the nodes clinically.
Sentinel lymph node biopsy is recommended by the American Society of Clinical Oncology and the Society of Surgical Oncology for patients with intermediate thickness cutaneous melanomas (Breslow thickness: 1–4 mm) of any anatomic site.
(http://ascopubs.org/doi/10.1200/JCO.2017.75.7724 Last Accessed: February 21, 2025)Level of Evidence/Strength of Recommendation: Intermediate/moderate
Further research led to the publication of a guideline (updated in 2017), jointly developed by the American Society of Clinical Oncology (ASCO) and the Society of Surgical Oncology (SSO), on the use of sentinel lymph node biopsy [162,163]. The following are the guideline recommendations [163,240]:
Sentinel lymph node biopsy is recommended for patients with cutaneous melanomas with Breslow thickness of 1–4 mm (intermediate thickness) at any anatomic site.
Sentinel lymph node biopsy may be recommended for staging purposes and to facilitate regional disease control for patients with melanomas that are T4 or >4 mm in Breslow thickness (thick).
There is insufficient evidence to support routine sentinel lymph node biopsy for patients with melanomas that are T1a or <0.8 mm (thin, nonulcerated).
Sentinel lymph node biopsy should be considered for patients with melanomas who are T1b or 0.8–1.0 mm in Breslow thickness, particularly those with high- risk features (e.g., ulceration and/or mitotic rate ≥1/mm2).
Completion of lymph node dissection is recommended for all patients with a positive sentinel lymph node biopsy.
The recommendations in the 2025 version of the NCCN guidelines are similar to those in the 2017 ASCO/SSO guidelines. The NCCN expert panel agrees that routine sentinel lymph node biopsy is not recommended for thin melanomas (<0.8 mm) and notes that a discussion of sentinel lymph node biopsy should be considered for melanomas that are 0.8–1.0 mm thick due to the 5% to 10% probability of a positive biopsy result [132,240]. The NCCN states that other factors (such as ulceration) should be considered when deciding on sentinel lymph node biopsy for T1b melanomas; additionally, the NCCN cites a mitotic index >2/mm2 (particularly with younger age) and lymphovascular invasion as other high-risk features [132]. Complete lymph node dissection is recommended when the sentinel node is positive and also when disease is clinically evident in one or more nodes [132]. The NCCN advises forgoing sentinel lymph node biopsy, even for recommended stages, if the patient is unfit or unwilling to act on biopsy results (e.g., additional monitoring, further disease treatment).
Despite its value as a staging tool and the available guidelines, sentinel lymph node biopsy has been underused, especially for patients older than 65 years of age, minority populations, patients with melanomas on the trunk and head and neck, and patients in some geographic areas [164,165]. Even when sentinel lymph node biopsy is done, appropriate dissection does not always follow. A 2008 study of practice patterns showed that complete dissection was done in approximately half of patients in whom disease was found in the sentinel node [166].
The prognosis for melanomas is related to the stage of disease at the time of diagnosis, the anatomic site, the sex of the patient, and other tumor characteristics. A poorer prognosis has been associated with melanomas diagnosed at a later stage; with those located on the head, neck, and trunk; and for those in men [25]. For metastatic disease, the prognosis is better for patients with metastasis to soft tissues or lymph nodes than for those with metastasis to the brain or liver. The five-year survival rate ranges from 99.4% for localized melanoma to 29.8% for distant disease (Table 12) [167]. As stated, survival rates are lower for racial/ethnic minority populations [27,47,127].
Follow-up, including the search for second primary melanomas, is crucial after treatment for melanoma, and the intervals depend on several factors, including thickness of the lesion and patient risk factors. The American Academy of Dermatology suggests follow-up one to four times per year for two years and one to two times per year thereafter [93]. The NCCN offers guidelines for follow-up based on stage of disease (Table 13) [132]. Follow-up should include emphasis on self-examination of the skin and lymph nodes [93,132]. Family members of patients with melanoma should be screened yearly.
NATIONAL COMPREHENSIVE CANCER NETWORK (NCCN) RECOMMENDATIONS FOR FOLLOW-UP AFTER TREATMENT FOR MELANOMA
| Clinical/Pathologic Stage | Follow-Up |
|---|---|
| Stage 0 (in situ) | Skin examination and surveillance annually for life |
| Stage IA–IIA | History and physical exam (with emphasis on lymph nodes and skin) every 6 to 12 months for five years, then annually as clinically indicated. Routine laboratory testing or imaging studies to screen for asymptomatic recurrent or metastatic disease is not recommended. |
| Stage IIB–IV | History and physical exam (with emphasis on lymph nodes and skin) every 3 to 6 months for two years, then every 3 to 12 months for three years, then annually as clinically indicated. Chest x-ray and other imaging studies may be considered to screen for recurrent/metastatic disease every 3 to 12 months. Routine laboratory testing or imaging studies to screen for asymptomatic recurrent or metastatic disease is not recommended after three to five years. |
Skin cancer screening practices vary considerably, and screening rates are generally low, even among individuals at high risk for skin cancer. The reported rates for full body skin examinations done during routine physician care have ranged from 15% to 60% [81,122]. Of 32,000 adults who participated in the 2000 or 2005 National Health Interview Survey (HINTS) cancer control supplements, 8% said they had had a skin examination within the past 12 months, although 70% had seen a physician during that time; 15% of the respondents reported ever having a skin cancer examination [168]. The rate of skin cancer screening was lower for individuals who had high-risk occupations (i.e., increased exposure to UV rays) than for individuals who had low-risk occupations [168]. An analysis of National Health Interview Survey Cancer Control Supplement data from 2010 showed that screening rates were higher among the elderly, the fair-skinned, those reporting sunburn(s), and those with a family history of skin cancer [169]. Another study found that the majority of those who seek screening are women [176]. Of the estimated 104.7 million (51.1%) U.S. adults with at least one risk factor for developing melanoma, only 24% reported at least one total body skin examination by a physician [169].
Several issues have been reported to be barriers to physician skin examinations [122]. Lack of time is the number-one barrier, cited by 42% of dermatologists and 70% of primary care providers [122]. Involving other practice staff, such as nurse practitioners and physician assistants, can help ease this burden. Other barriers included poor or no training and lack of confidence [122]. In a study of medical students, 69% said that there was insufficient attention to skin cancer examinations in their medical training. Of the respondents, 23% had never observed a skin cancer examination and 27% had never been trained to perform such an examination [40]. As a result, only 28% rated themselves as somewhat or very skilled in the procedure. Education to enhance the knowledge and diagnostic skills of medical students as well as primary care providers has led to increased confidence and diagnostic accuracy [122]. More initiatives such as these can help further improve early detection.
Another barrier to screening is the lack of scientific evidence to support the practice [122]. In general, there is insufficient evidence to recommend periodic screening for melanoma in the general adult population. This was the conclusion of the U.S. Preventive Services Task Force (USPSTF) when it updated its statement in 2016 [170,171]. The Task Force noted that there was "fair" evidence that screening by clinicians was "moderately accurate" in detecting melanoma, but that there was insufficient evidence to determine that screening reduces the morbidity or mortality rates associated with skin cancer [170]. Potential harms of detection and early treatment were noted to be misdiagnosis, overdiagnosis, and harm related to biopsy and treatment [170]. This same conclusion has been drawn by many other organizations, including the American Academy of Family Physicians and the NCI [172,173]. The HINTS study indicated that routine screening through total-body skin exam for melanomas and nonmelanomas is also not recommended, as there is inadequate evidence to suggest that population-wide screening would be effective [241].
Other professional organizations have set forth recommendations that primarily target individuals at high risk for melanoma. The American Academy of Dermatology suggests an annual skin examination by a dermatologist, especially for adults who have known risk factors, such as a history of substantial sun exposure or a family history of skin cancer [177]. The Academy also offers the Melanoma/Skin Cancer Screening Program, which provides free skin examinations by volunteer dermatologists [177]. The Skin Cancer Foundation also recommends annual screening by a dermatologist [174]. The American Cancer Society has set forth definitive screening recommendations: skin examination by a physician as part of a cancer check-up every three years for individuals 20 to 39 years of age and annually beginning at 40 years of age [178]. The American Cancer Society, American Academy of Dermatology, Skin Cancer Foundation, and the NCI recommend that individuals perform self-examinations, usually at four-to eight-week intervals [172,174,177,178].
Since the USPSTF issued its update, studies have shown that both physician examination and self-examination can lead to earlier detection, when cure is more likely. In a study of 126 asymptomatic individuals with melanomas, skin examinations by dermatologists were associated with significantly thinner melanomas (less than 1.0 mm) and an increasing likelihood of the lesion being in situ [179]. In a case-control study, skin cancer screening was associated with a 38% higher likelihood of being diagnosed with a thin melanoma (0.75 mm or less) [180]. An increased rate of detection of melanomas when they are thinner would seem to support an association with better outcomes, given that tumor thickness is an important prognostic factor. There has been a call for a national plan to enhance prevention and detection by providing screening as a health benefit, expanding outreach and education, and advocating for legislation to support screening and education [181].
The U.S. Preventive Services Task Force recommends counseling young adults, adolescents, children, and parents of young children about minimizing exposure to UV radiation for persons 6 months to 24 years of age with fair skin types to reduce their risk of skin cancer.
(https://jamanetwork.com/journals/jama/fullarticle/2675556 Last Accessed: February 21, 2025)Strength of Recommendation: B (There is high certainty that the net benefit is moderate or there is moderate certainty that the net benefit is moderate to substantial.)
Patient education is the cornerstone of efforts to prevent skin cancer. The USPSTF recommends counseling for children, adolescents, young adults, and parents of young children to minimize UV exposure among those 10 to 24 years of age (particularly those with "fair skin"), thereby reducing the risk of skin cancer [182]. The USPSTF found insufficient evidence to assess the balance of benefits and harms of such counseling for adults older than 24 years of age, but recommends selective counseling based on presence of risk factors for skin cancer [182]. Talking to patients about ways to protect themselves from UV rays should be carried out, with several points of emphasis (Table 14). Every summer, the consumer media is inundated with information on reducing the risks of sun exposure, and physicians should reinforce this information. Although Healthy People 2030 sets no targets regarding protective measures that may reduce the risk of skin cancer, healthcare providers should work toward attaining the goal of increasing, from 70.8%, the proportion of adults who usually or always apply sunscreen with a sun protection factor (SPF) of 15 or higher, wear protective clothing, or seek shade [183]. Men are significantly less likely to use sunscreen than women [175,183].
POINTS OF EMPHASIS FOR PATIENT EDUCATION ON PREVENTION OF SKIN CANCERS
| Use of Sunscreen | |||||||||
| |||||||||
| Other Protection from UV Rays | |||||||||
| |||||||||
| Self-Examination | |||||||||
|
Learn how to:
| |||||||||
| Other | |||||||||
|
Efforts to educate patients should emphasize three key points: protection from UV rays, the importance of self-examinations and examination of family members, and the need to monitor existing moles for changes.
Given the high association between sun exposure and increased risk for skin cancer, many skin cancers could be prevented through enhanced protection from UV rays. Skin cancer prevention campaigns have emphasized several behaviors to protect against UV rays [183,184,185]:
Use sunscreen
Seek shade
Wear a wide-brimmed hat
Wear protective clothing (long-sleeved shirt and/or long pants)
Avoid the sun between 10 a.m. and 4 p.m.
The rates of these regular sun-safety practices are low, despite the clear link between UV protection and lower rates of skin cancer, as well as the substantial number of initiatives to heighten awareness about the importance of UV protection [5,186,187]. In the 2021 National Cancer Institute's Cancer Trends Progress Report, approximately 65% of respondents reported not regularly using sunscreen, and approximately 60% did not wear protective clothing or seek shade (Figure 5) [183].
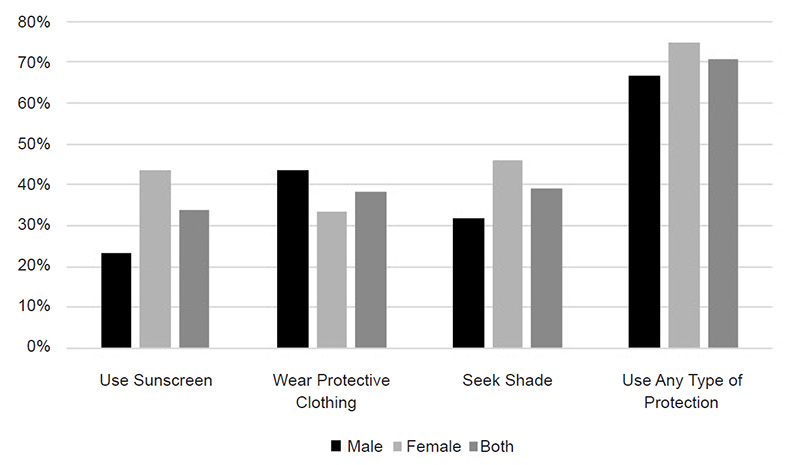
Many individuals remember to use sunscreen when they intend to be exposed to the sun, but they do not use sunscreen routinely [5]. The low rate of sunscreen use and other sun protections is reflected in the rates of sunburn in the United States. Data from 2020 were examined and showed that 64.4% of high school students and 29.1% of all adult respondents had at least one sunburn during the preceding year [188]. In adults, the rates were highest among non-Hispanic White individuals (41.1%), followed by Hispanic (14.4%), and Black individuals (5.6%) [188]. Sunburns were found to be equally common in adult men (29.5%) and women (28.9%), but higher (40.6%) in younger adults (18 to 24 years of age) and in individuals more prone to sunburn [188,189].
Some have claimed that the use of sunscreen actually increases the risk for melanoma, but this finding was not supported by an analysis of 18 case-controlled studies [190]. There is also debate regarding the effectiveness of sunscreen in reducing skin cancer, and no study has shown that the use of sunscreen reduces the risk of basal cell carcinoma. A few studies have shown that sunscreen reduces the incidence of squamous cell carcinoma and melanoma, but large-scale reliable information is lacking and these studies are contradicted in other literature [158,171,175,191,192].
It has been postulated that sunscreen use has not reduced the rates of skin cancer because individuals who use sunscreen may remain in the sun longer because they feel protected. To test this, researchers provided vacationers with free sunscreen that was labeled as high protection or basic protection; the high protection sunscreen had a sun protection factor (SPF) of either 12 or 40, while the basic protection had an SPF of 12. The researchers found that the higher SPF did not influence the amount of time in the sun [193]. A more plausible reason for continued high rates of skin cancer is the widespread inappropriate use of sunscreens. In one study, 73% of individuals who used sunscreen still sunburned [194].
Protection behaviors are especially crucial for individuals with risk factors for skin cancers related to UV exposure, such as fair complexion, light-colored eyes, blond or red hair, and tendency to burn or freckle with exposure to the sun. Individuals with these characteristics have been shown to be more likely to use sun protection than other individuals and may be receptive to educational interventions on prevention [187]. Protection from the sun is also crucial for children, as they are at highest risk for sunburn and because they may receive as much as two to three times the sun exposure as adults [195]. Special attention should be given to children with a family history of skin cancer. One study found that frequent sunburns, suboptimal use of sunscreen, and high rates of tanning salon use were evident among children of mothers with a personal or family history of skin cancer [196]. Reinforcing sun protection habits in young children can enhance the likelihood that the habits will be continued through adolescence and adulthood [197]. The appropriate use of sunscreen in childhood may reduce the lifetime risk for nonmelanoma skin cancer by up to 78% [198].
Fact sheets on prevention targeted to different grade levels are part of the Centers for Disease Control and Prevention (CDC) Sun Safety Resource Toolkit, which is available on the CDC website.
Healthcare professionals should also talk to their patients about the hazard of indoor tanning facilities, targeting those patients who are most likely to use such facilities. According to the 2018 HINTS, 87% of individuals indicated that their physician had not talked them about reducing rates of exposure to the sun or indoor tanning devices [199]. As noted, rates of indoor tanning have been decreasing since the early 2000s, but in 2015, 3.5% of adults and 7.3% of adolescents still used indoor tanning [67,68,69]. The highest rate of indoor tanning is among White women 18 to 21 years of age (20.4%) [69]. The danger of indoor tanning for youths has led at least 44 states to establish legislation restricting youth's access to such facilities. In addition, 19 states and the District of Columbia have passed legislation banning the use of tanning beds for all children younger than 18 years of age [71]. Most tanning facilities require parental consent for minors (younger than 18 years of age), and healthcare providers should encourage parents to decline giving consent. The FDA continues to review the growing body of literature linking UV radiation exposure from tanning devices and skin cancer in consideration of stricter regulations overall. In 2014, the FDA changed labeling requirements for sunlamp products and ultraviolet or UV lamps used in indoor tanning salons from low-risk to moderate-risk devices. The agency has also required the products to carry a black box warning. The warning must be visible to consumers and must state that the product should not be used for people younger than 18 years of age [206].
Self-examination has been estimated to reduce melanoma-related mortality by 63%, and healthcare providers should encourage their patients, especially those at high risk for skin cancer, to perform self-examination regularly [207]. Knowledge of skin cancer risk and of the importance of early detection have been associated with increased likelihood of performing self-examination, and a diagnosis of skin cancer within the previous three years is a strong predictor [122]. Instructional videos, sample photographs, and hand mirrors have been shown to enhance performance of self-examination [208]. Healthcare providers should talk to their patients about the importance of monitoring moles or skin lesions over time and about the indicators of melanoma, describing the ABCDE criteria. Determining the A, B, C, and E criteria from the ABCDE rule may be difficult for some individuals, but training can enhance skills [209].
Problems with eyesight and physical mobility may make it difficult for some individuals, especially older persons, to carry out self-examination. Healthcare providers should engage other family members in discussions about self-examination and encourage spouses and partners to help with skin examinations. Educational programs directed at the individual as well as a partner (a person living with the individual) have been found to be more effective than programs directed solely at the individual [210].
Because of differences in culture, literacy, and learning preferences, individual needs for educational resources vary. All these needs should be addressed to effectively convey the importance of strategies to prevent skin cancer.
Culture, reading literacy, and health literacy (i.e., the ability to understand health information and make informed health decisions) are all factors to consider when talking to patients about skin cancer and its prevention. The disparities in survival attributable to advanced stage at the time of diagnosis call for enhanced awareness in minority populations about their risk for skin cancers and about how the site of skin cancers may differ from traditional sites (i.e., areas of the body not exposed to sun). The rates of sunburn reported for minority populations also suggest that more education is needed about the importance of sun protection.
Compounding the issue of educating individuals about skin cancers and prevention are the lower rates of health literacy among populations at high risk [211]. The National Assessment of Adult Literacy estimated that only 12% of adults have "proficient" health literacy and 14% have "below basic" health literacy, and rates of health literacy are especially low among ethnic minority populations and individuals older than 60 years of age [211,212]. In addition, according to U.S. Census Bureau data from 2023, almost 69 million Americans speak a language other than English in the home, with approximately 26.3 million of them (8.4% of the population) speaking English less than "very well" [213].
Healthcare professionals should assess their patients' literacy level and understanding and talk with them in a manner that increases the likelihood of understanding. For example, clinicians should use plain language in their discussions with patients who have low literacy or limited English proficiency. They should ask patients to repeat pertinent information in their own words to confirm understanding [214]. Reinforcement with the use of low-literacy or translated educational materials is helpful.
It has been suggested that when patients are first evaluated, they should be asked what language is spoken at home and if they speak English "very well" (if the healthcare professional is English-speaking) [215]. In addition, physicians should ask what language they prefer for their medical care information, as some patients prefer their native language even though they have said they can understand and discuss symptoms in English [215].
"Ad hoc" interpreters (i.e., family members, friends, bilingual staff members) are often used instead of professional interpreters for a variety of reasons, including convenience and cost. Physicians should check with their state's health officials about the use of ad hoc interpreters, as several states have laws about who can interpret medical information for a patient [216]. Even when allowed by law, the use of a patient's family member or friend as an interpreter should be avoided, as the patient may not be as forthcoming with information and the family member or friend may not remain objective [216]. Children should especially be avoided as interpreters, as their understanding of medical language is limited and they may filter information to protect their parents or other adult family members [216]. Individuals with limited English language skills have indicated a preference for professional interpreters rather than family members [217].
Most important, perhaps, is the fact that clinical consequences are more likely with ad hoc interpreters than with professional interpreters [218]. A systematic review of the literature showed that the use of professional interpreters facilitates a broader understanding and leads to better clinical care than the use of ad hoc interpreters. Many studies have demonstrated that the lack of an interpreter for patients with limited English proficiency compromises the quality of care and that the use of professional interpreters improves communication (errors and comprehension), utilization, clinical outcomes, and patient satisfaction with care [219,220].
A professional interpreter is more than a neutral party who communicates information between two parties. An interpreter is an active agent, negotiating between two cultures and assisting in promoting culturally competent communication and practice [221]. In this more active role, the interpreter's behavior is also influenced by a host of cultural variables such as gender, class, religion, educational differences, and power/authority perceptions of the patient [221].
Healthcare providers should have educational resources available in a variety of formats and media, as learning styles differ among adults. Depending on the individual, learning may be optimal with printed materials, illustrations, videos, interactive tutorials, online resources, or a combination of resources. Asking an individual how he or she prefers to learn can help healthcare providers select the best resources. A variety of government agencies and professional organizations have developed educational materials about skin cancers. These resources, available in print and online, are often available in languages other than English (Table 15).
EDUCATIONAL RESOURCES FOR PATIENTS
| Resource | Description | |||||
|---|---|---|---|---|---|---|
| Educational pamphlets on melanomas and nonmelanomas | |||||
| Overviews of melanomas and nonmelanomas, as well as guidelines for sun safety and skin cancer prevention; information available in Spanish (https://es.familydoctor.org/condicion/cancer-de-piel) | |||||
|
| |||||
|
| |||||
| Comprehensive information on melanoma, including research and advocacy efforts; resources include chats, educational teleconferences, and details on special events | |||||
|
| |||||
|
| |||||
|
|
The Internet has become a primary source of health information; approximately 80.2% of respondents to the 2017 HINTS said they used the Internet in the past 12 months to search for health or medical information [199]. However, in a study of 74 websites offering information on melanoma, researchers found that most websites had incomplete information and 14% contained inaccuracies [223]. The sites were likely to lack complete basic information, such as that related to risk factors, diagnosis, treatment, prevention, and prognosis. Clinicians can help ensure that their patients gain accurate information from online sources by guiding patients to authoritative websites.
Basal cell carcinoma, squamous cell carcinoma, and melanoma comprise the majority of skin cancers. The risk for skin cancers varies among several populations, with the highest rates found for White men older than 50 years of age, and lower rates among the Black, American Indian, Hispanic, and Asian populations than for White individuals. Also increasing risk are immunosuppression, characteristics that predispose the skin to sunburn (e.g., light complexion, light-colored eyes and hair), and a personal or family history of skin cancer.
Early treatment of nonmelanomas and melanoma is integral to cure, making it essential for patients to know how to detect suspicious lesions and to understand the importance of seeking medical attention for such lesions. In turn, primary care providers should enhance their abilities to detect skin cancer, especially given that formal education and training has not been strong in this area. The primary challenges in diagnosing skin cancers are to distinguish between benign and malignant lesions and to identify lesions with malignant potential. The clinical characteristics and use of the ABCDE method are key to diagnosis. Several treatment options are available for nonmelanomas, and the type of treatment is selected on the basis of several factors, such as tumor characteristics, patient age, medical status, and patient preference. Guidelines are available for both nonmelanomas and melanoma. For melanoma, the goal of treatment is to remove all malignant tissue and minimize local recurrence. Sentinel lymph node biopsy, an underused procedure, can help identify individuals who will benefit from lymph node dissection and those who can avoid the procedure (and its morbidity) without compromising survival.
Although the USPSTF has determined that there is insufficient evidence to recommend periodic screening for melanoma in adults, annual examinations by a healthcare provider, along with monthly self-examinations, is prudent. Effective patient education, particularly about the harmful effects of UV radiation from natural and artificial UV radiation and about early detection and treatment, can substantially reduce the morbidity and mortality associated with skin cancers.
| Centers for Disease Control and Prevention |
| Sun Safety Facts |
| https://www.cdc.gov/skin-cancer/sun-safety |
| National Cancer Institute |
| Melanoma Risk Assessment Tool |
| https://mrisktool.cancer.gov |
| Skin Cancer Foundation |
| https://www.skincancer.org |
1. American Cancer Society. Cancer Facts and Figures 2025. Available athttps://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2025/2025-cancer-facts-and-figures-acs.pdf. Last accessed February 10, 2025.
2. Skin Cancer Foundation. Skin Cancer Facts. Available athttps://www.skincancer.org/skin-cancer-information/skin-cancer-facts. Last accessed February 10, 2025.
3. Eide MJ, Krajenta R, Johnson D, et al. Identification of patients with nonmelanoma skin cancer using health maintenance organization claims data. Am J Epidemiol. 2010;171(1):123-128.
4. Edwards BK, Noone AM, Mariotto AB, et al. Annual report to the nation on the status of cancer, 1975–2014, featuring survival. J Natl Cancer Inst. 2017;109(9):1-22.
5. Stern RS. Prevalence of a history of skin cancer in 2007: results of an incidence-based model. Arch Dermatol. 2010;146(3):279-82.
6. American Academy of Dermatology. Skin Cancer. Available at https://www.aad.org/media/stats/conditions/skin-cancer. Last accessed February 10, 2025.
7. Jerant AF, Johnson JT, Sheridan CD, Caffrey TJ. Early detection and treatment of skin cancer. Am Fam Phys. 2000;62(2):357-368.
8. Bader RS, Kennedy AS, Santacroce L, Diomede L. Basal Cell Carcinoma. Available at https://emedicine.medscape.com/article/ 276624-overview. Last accessed February 10, 2025.
9. Walter J. Cancer of the skin. In: Kasper D, Fauci A, Hauser S, Longo D, Jameson J, Loscalzo J. Harrison's Principles of Internal Medicine. 19th ed. New York, NY: McGraw-Hill Companies; 2012.
10. National Cancer Institute. Kaposi Sarcoma Treatment (PDQ). Available at https://www.cancer.gov/types/soft-tissue-sarcoma/hp/kaposi-treatment-pdq. Last accessed February 12, 2025.
11. Dinh V, Feun L, Elgart G, Savaraj N. Merkel cell carcinomas. Hematol Oncol Clin N Am. 2007;21(3):527-544.
12. Pearson JM. Dermatologic Manifestations of Merkel Cell Carcinoma. Available at https://emedicine.medscape.com/article/1100917-overview. Last accessed February 12, 2025.
13. Paulson KG, Park SY, Vandeven NA, et al. Merkel cell carcinoma: current U.S. incidence and projected increases based on changing demographics. J Am Acad Dermatol. 2018;78(3):457-463.
14. National Cancer Institute. Merkel Cell Carcinoma Treatment (PDQ). Available at https://www.cancer.gov/types/skin/hp/merkel-cell-treatment-pdq. Last accessed February 11, 2025.
15. Lewis KG, Weinstock MA, Weaver AL, Otley CC. Adjuvant local irradiation for Merkel cell carcinoma. Arch Dermatol. 2006;142(6):693-700.
16. Scotto J, Kopf AW, Urbach F. Non-melanoma skin cancer among Caucasians in four areas of the United States. Cancer. 1974;34(4):1333-1338.
17. Arora A, Attwood J. Common skin cancers and their precursors. Surg Clin N Am. 2009;89(3):703-712.
18. Skin Cancer Foundation. Squamous Cell Carcinoma: Causes and Risk Factors. Available at https://www.skincancer.org/skin-cancer-information/squamous-cell-carcinoma/scc-causes-and-risk-factors. Last accessed February 11, 2025.
19. National Cancer Institute Surveillance, Epidemiology, and End Results Program. Melanoma of the Skin: Recent Trends in SEER Age-Adjusted Incidence Rates, 2000–2021. Available at https://seer.cancer.gov/explorer/application.html. Last accessed February 11, 2025.
20. National Cancer Institute Surveillance, Epidemiology, and End Results Program. Melanoma of the Skin: SEER Incidence Rates by Age at Diagnosis, 2017–2021. Available at https://seer.cancer.gov/statistics-network/explorer/application.html?site=53&data_type=1&graph_type=3&compareBy=sex&chk_sex_3=3&chk_sex_2=2&rate_type=1&race=1&advopt_precision=1&advopt_show_ci=on&hdn_view=0&advopt_show_apc=on&advopt_display=2. Last accessed February 11, 2025.
21. National Cancer Institute Surveillance, Epidemiology, and End Results Program. Cancer Stat Facts: Who Gets This Cancer? Available at http://seer.cancer.gov/statfacts/html/melan.html. Last accessed February 11, 2025.
22. National Cancer Institute National Childhood Cancer Registry Explorer. Melanomas: 5-Year Age-Adjusted Incidence Rates, 2017-2021. Available at https://nccrexplorer.ccdi.cancer.gov/application.html?site=1104&data_type=1&graph_type=10&compareBy=sex&chk_sex_1=1&chk_sex_3=3&chk_sex_2=2&series=9&race=1&age_range=1&advopt_precision=1&advopt_show_ci=on. Last accessed February 11, 2025.
23. American Cancer Society. Key Statistics for Melanoma Skin Cancer. Available at https://www.cancer.org/cancer/melanoma-skin-cancer/about/key-statistics.html. Last accessed February 10, 2025.
24. Hu S, Soza-Vento RM, Parker DF, Kirsner RS. Comparison of stage at diagnosis of melanoma among Hispanic, black, and white patients in Miami-Dade County, Florida. Arch Dermatol. 2006;142(6):704-708.
25. Brenner M, Hearing VJ. The protective role of melanin against UV damage in human skin. Photochem Photobiol. 2008;84(3): 539-549.
26. Montagna W, Carlisle K. The architecture of black and white facial skin. J Am Acad Dermatol. 1991;24(6 pt 1):929-937.
27. Battie C, Gohara M, Verschoore M, Roberts W. Skin cancer in skin of color: an update on current facts, trends, and misconceptions. J Drugs Dermatol. 2013;12(2):194-198.
29. Edwards BK, Ward E, Eheman C, et al. Annual report to the nation on the status of cancer, 1975–2006, featuring colorectal cancer trends and impact of interventions (risk factors, screening, and treatment) to reduce future rates. Cancer. 2010;116(3):544-573.
31. Karagas MR, Nelson HH, Sehr P, et al. Human papillomavirus infection and incidence of squamous cell and basal cell carcinomas of the skin. J Natl Cancer Inst. 2006;98(6):389-395.
32. Yoon J, Roenigk RK. Skin cancers. In: Lang RS, Hensrud DD. Clinical Preventive Medicine. 2nd ed. Chicago, IL: American Medical Association Press; 2004: 561-570.
34. Perkins JL, Liu Y, Mitby PA, et al. Nonmelanoma skin cancer in survivors of childhood and adolescent cancer: a report from the Childhood Cancer Survivor Study. J Clin Oncol. 2005;23(16):3733-3741.
35. Kricker A, Armstrong BK, English DR. Sun exposure and non-melanocytic skin cancer. Cancer Causes Control. 1994;5(4):367-392.
36. National Cancer Institute Surveillance Epidemiology and End Results Program. Browse the SEER Cancer Statistics Review, 1975–2015. Risk of Developing/Dying: Table 16.12: Melanoma of the Skin (Invasive). Available at https://seer.cancer.gov/csr/1975_2015/browse_csr.php?sectionSEL=16&pageSEL=sect_16_table.12. Last accessed February 11, 2025.
38. Saiyed FK, Hamilton EC, Austin MT. Pediatric melanoma: incidence, treatment, and prognosis. Pediatric Health Med Ther. 2017;8:39-45.
39. Christenson LJ, Borrowman TA, Vachon CM, et al. Incidence of basal cell and squamous cell carcinomas in a population younger than 40 years. JAMA. 2005;294(6):681-690.
40. Moore MM, Geller AC, Zhang Z, et al. Skin cancer examination teaching in US medical education. Arch Dermatol. 2006;142(4):439-444.
41. National Cancer Institute Surveillance Epidemiology and End Results Program. Browse the SEER Cancer Statistics Review, 1975–2015. Relative Survival (Percent) by Year of Diagnosis, All Races, Males and Females: Table 16.9: Melanoma of the Skin (Invasive). Available at https://seer.cancer.gov/csr/1975_2015/browse_csr.php?sectionSEL=16&pageSEL=sect_16_table.09. Last accessed February 11, 2025.
42. Karia PS, Han J, Schmults CD. Cutaneous cell carcinoma: estimated incidence of disease, nodal metastasis, and deaths from disease in the United States, 2012. J Am Acad Dermatol. 2013;68(6):957-966.
43. National Cancer Institute Surveillance Epidemiology and End Results Program. Browse the SEER Cancer Statistics Review, 2000–2021. Age-Adjusted Rates and Trends by Race/Ethnicity and Sex, 2000–2021. Available at https://seer.cancer.gov/statistics-network/explorer/application.html?site=53&data_type=4&graph_type=2&compareBy=race&chk_race_1=1&chk_race_3=3&relative_survival_interval=5&sex=1&age_range=1&stage=101&advopt_precision=1&advopt_show_ci=on&hdn_view=0&advopt_show_apc=on&advopt_display=2. Last accessed February 11, 2025.
44. U.S. Department of Health and Human Services National Toxicology Program. 15th Report on Carcinogens. Available at https:// ntp.niehs.nih.gov/whatwestudy/assessments/cancer/roc/index.html. Last accessed February 11, 2025.
45. U.S. Department of Health and Human Services. The Surgeon General's Call to Action to Prevent Skin Cancer. Washington, DC: U.S. Department of Health and Human Services, Office of the Surgeon General; 2014.
46. Qureshi AA, Laden F, Colditz GA, Hunter DJ. Geographic variation and risk of skin cancer in U.S. women: differences between melanoma, squamous cell carcinoma, and basal cell carcinoma. Arch Intern Med. 2008;168(5):501-507.
47. Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancer statistics, 2009. CA Cancer J Clin. 2009;59(4):225-249.
48. Wu S, Han J, Vleugels RA, et al. Cumulative ultraviolet radiation flux in adulthood and risk of incident skin cancers in women. Br J Cancer. 2014;110:1855-1861.
49. Rigel DS. Cutaneous ultraviolet exposure and its relationship to the development of skin cancer. J Am Acad Dermatol. 2008;58(5):S129-S132.
50. Neale RE, Barnes PW, Robson TM, et al. Environmental effects of stratospheric ozone depletion, UV radiation, and interactions with climate change: UNEP Environmental Effects Assessment Panel, Update 2020. Photochem Photobiol Sci. 2021;20(1):1-67.
51. Godar DE, Urbach F, Gasparro FP, van der Leun JC. UV doses of young adults. Photochem Photobiol. 2003;77(4):453-457.
52. Green AC, Wallingford SC, McBride P. Childhood exposure to ultraviolet radiation and harmful skin effects: epidemiological evidence. Prog Biophys Mol Biol. 2011;107(3):349-355.
53. Kricker A, Armstrong BK, English DR, Heenan PJ. Does intermittent sun exposure cause basal cell carcinoma? A case-control study in Western Australia. Int J Cancer. 1995;60(4):489-494.
54. Zanetti R, Rosso S, Martinez C, et al. Comparison of risk patterns in carcinoma and melanoma of the skin in men: a multi-centre case-case-control study. Br J Cancer. 2006;94(5):743-751.
55. Claerhout S, Van Laethem A, Agostinis P, Garmyn M. Pathways involved in sunburn cell formation: deregulation in skin cancer. Photochem Photobiol Sci. 2006;5(2):199-207.
56. Chen YC, Christiani DC, Su HJ, et al. Early-life or lifetime sun exposure, sun reaction, and the risk of squamous cell carcinoma in an Asian population. Cancer Causes Control. 2010;21(5):771-776.
57. Beitner H, Norell SE, Ringborg U, Wennersten G, Mattson B. Malignant melanoma: aetiological importance of individual pigmentation and sun exposure. Br J Dermatol. 1990;122(1):43-51.
58. Holly EA, Aston DA, Cress RD, Ahn DK, Kristiansen JJ. Cutaneous melanoma in women. I. Exposure to sunlight, ability to tan, and other risk factors related to ultraviolet light. Am J Epidemiol. 1995;141(10):923-933.
59. Osterlind A, Tucker MA, Stone BJ, Jensen OM. The Danish case-control study of cutaneous malignant melanoma. II. Importance of ultraviolet-light exposure. Int J Cancer. 1988;42(3):319-324.
60. Ródenas JM, Delgado-Rodríguez M, Herranz MT, Tercedor J, Serrano S. Sun exposure, pigmentary traits, and risk of cutaneous malignant melanoma: a case-control study in a Mediterranean population. Cancer Causes Control. 1996;7(2):275-283.
61. Wolf P, Quehenberger F, Müllegger R, Stranz B, Kerl H. Phenotypic markers, sunlight-related factors and sunscreen use in patients with cutaneous melanoma: an Austrian case-control study. Melanoma Res. 1998;8(4):370-378.
62. Espinosa Arranz J, Sanchez Hernandez JJ, Bravo Fernandez P, et al. Cutaneous malignant melanoma and sun exposure in Spain. Melanoma Res. 1999;9(2):199-205.
63. Whiteman DC, Stickley M, Watt P, Hughes MC, Davis MB, Green AC. Anatomic site, sun exposure, and risk of cutaneous melanoma. J Clin Oncol. 2006;24(19):3172-3177.
64. Gandini S, Sera F, Cattaruzza MS, et al. Meta-analysis of risk factors for cutaneous melanoma. II. Sun exposure. Eur J Cancer. 2005;41(1):45-60.
65. Lew RA, Sober AJ, Cook N, Marvell R, Fitzpatrick TB. Sun exposure habits in patients with cutaneous melanoma: a case control study. J Dermatol Surg Oncol. 1983;9(12):981-986.
66. Pfahlberg A, Kölmel KF, Gefeller O, Febim Study Group. Timing of excessive ultraviolet radiation and melanoma: epidemiology does not support the existence of a critical period of high susceptibility to solar ultraviolet radiation-induced melanoma. Br J Dermatol. 2001;144(3):471-475.
67. Levine JA, Sorace M, Spencer J, Siegel DM. The indoor UV tanning industry: a review of skin cancer risk, health benefit claims, and regulation. J Am Acad Dermatol. 2005;53(6):1038-1044.
68. Guy GP, Berkowitz Z, Everett Jones S, Watson M, Richardson LC. Prevalence of indoor tanning and association with sunburn among youth in the United States. JAMA Dermatol. 2017;153(5):387-390.
69. Guy GP Jr, Watson M, Seidenberg AB, Hartman AM, Perna F. Trends in indoor tanning and its association with sunburn among U.S. adults. J Am Acad Dermatol. 2017;76(6):1191-1193.
70. Schulman JM, Fisher DE. Indoor ultraviolet tanning and skin cancer: health risks and opportunities. Curr Opin Oncol. 2009;21(2):144-149.
71. AIM at Melanoma Foundation. Indoor Tanning Restrictions for Minors. Available at https://www.aimatmelanoma.org/legislation-policy-advocacy/indoor-tanning/. Last accessed February 11, 2025.
72. Mayer JE. The window of opportunity for indoor tanning legislation. Transl Behav Med. 2014;4(4):434-435.
73. Centers for Disease Control and Prevention. Skin Cancer Prevention Progress Report 2018. Atlanta, GA: Centers for Disease Control and Prevention, U.S. Department of Health and Human Services; 2018.
74. Sexton M, Jones DB, Maloney ME. Histologic pattern analysis of basal cell carcinoma: study of a series of 1039 consecutive neoplasms. J Am Acad Dermatol. 1990;23(6 pt 1):1118-1126.
76. Stulberg DL, Crandell B, Fawcett RS. Diagnosis and treatment of basal cell and squamous cell carcinomas. Am Fam Phys. 2004;70(8):1481-1488.
78. Cassarino DS, Derienzo DP, Barr RJ. Cutaneous squamous cell carcinoma: a comprehensive clinicopathologic classification: part one. J Cutan Pathol. 2006;33(3):191-206.
79. Wagner RF Jr, Wagner D, Tomich JM, Wagner KD, Grande DJ. Diagnosis of skin disease: dermatologists vs. nondermatologists. J Dermatol Surg Oncol. 1985;11(5):476-479.
80. Centers for Disease Control and Prevention. National Center for Health Statistics: Ambulatory Care Use and Physician Office Visits. Available at https://www.cdc.gov/nchs/fastats/physician-visits.htm. Last accessed February 11, 2025.
81. Geller AC, O'Riordan DL, Oliveria SA, Valvo S, Teich M, Halpern AC. Overcoming obstacles to skin cancer examinations and prevention counseling for high-risk patients: results of a national survey of primary care physicians. J Am Board Fam Pract. 2004;17(6):416-423.
82. American Academy of Family Physicians. Family Medicine Facts. Table 12: Clinical Procedures Performed by Physicians at their Practice. Available at https://www.aafp.org/about/dive-into-family-medicine/family-medicine-facts/table12.html. Last accessed February 11, 2025.
83. Schwartz JL, Wang TS, Hamilton TA, Lowe L, Sondak VK, Johnson TM. Thin primary cutaneous melanomas: associated detection patterns, lesion characteristics, and patient characteristics. Cancer. 2002;95(7):1562-1568.
84. National Comprehensive Cancer Network. Clinical Practice Guidelines in Oncology. Squamous Cell Skin Cancer. V.2.2025. Available at https://www.nccn.org/professionals/physician_gls/pdf/squamous.pdf. Last accessed February 11, 2025.
85. Argenziano G, Soyer HP. Dermoscopy of pigmented skin lesions: a valuable tool for early diagnosis of melanoma. Lancet Oncol. 2001;2(7):443-449.
86. Argenziano G, Soyer HP, Chimenti S, et al. Dermoscopy of pigmented skin lesions: results of a consensus meeting via the Internet. J Am Acad Dermatol. 2003;48(5):679-693.
87. Carli P, de Giorgi V, Chiarugi A, et al. Addition of dermoscopy to conventional naked-eye examination in melanoma screening: a randomized study. J Am Acad Dermatol. 2004;50(5):683-689.
88. Carli P, De Giorgi V, Crocetti E, et al. Improvement of malignant/benign ratio in excised melanocytic lesions in the "dermoscopy era:" a retrospective study 1997–2001. Br J Dermatol. 2004;150(4):687-692.
89. Argenziano G, Puig S, Zalaudek I, et al. Dermoscopy improves accuracy of primary care physicians to triage lesions suggestive of skin cancer. J Clin Oncol. 2006;24(12):1877-1882.
90. Raasch BA, Buettner PG, Garbe C. Basal cell carcinoma: histological classification and body-site distribution. Br J Dermatol. 2006;155(2):401-407.
91. Benedetto AV, Benedetto EA, Griffin TD. Basal cell carcinoma presenting as a large pore. J Am Acad Dermatol. 2002;47(5):727-732.
92. Gold MH, Nestor MS. Current treatments of actinic keratosis. J Drugs Dermatol. 2006;5(2 suppl):17-25.
93. Swetter SM, Tsao H, Bichakjian CK, et al. Guidelines of care for the management of primary cutaneous melanoma. J Am Acad Dermatol. 2019;80(1):208-250.
94. Amin MB, Edge S, Greene F, et al. (eds). AJCC Cancer Staging Manual. 8th ed. New York, NY: Springer; 2017.
95. Smeets NW, Krekels GA, Ostertag JU, et al. Surgical excision vs. Mohs' micrographic surgery for basal-cell carcinoma of the face: randomised controlled trial. Lancet. 2004;364(9447):1766-1772.
96. Bath FJ, Bong J, Perkins W, Williams HC. Interventions for basal cell carcinoma of the skin. Cochrane Database Syst Rev. 2003;(2):CD003412.
97. Essers BA, Dirksen CD, Nieman FH, et al. Cost-effectiveness of Mohs micrographic surgery vs. surgical excision for basal cell carcinoma of the face. Arch Dermatol. 2006;142(2):187-194.
98. Nestor MS, Gold MH, Kauvar AN, et al. The use of photodynamic therapy in dermatology: results of a consensus conference. J Drugs Dermatol. 2006;5(2):140-154.
99. Braathen LR, Szeimies RM, Basset-Seguin N, et al. Guidelines on the use of photodynamic therapy for nonmelanoma skin cancer: an international consensus. J Am Acad Dermatol. 2007;56(1):125-143.
100. Rhodes AR, Weinstock MA, Fitzpatrick TB, Mihm MC Jr, Sober AJ. Risk factors for cutaneous melanoma: a practical method of recognizing predisposed individuals. JAMA. 1987;258(21):3146-3154.
101. Bader RS. Basal Cell Carcinoma Treatment and Management. Available at https://emedicine.medscape.com/article/276624-treatment. Last accessed February 12, 2025.
102. Bath-Hextall F, Bong J, Perkins W, Williams H. Interventions for basal cell carcinoma of the skin: systematic review. BMJ. 2004;329(7468):705.
103. National Comprehensive Cancer Network. Clinical Practice Guidelines in Oncology. Basal Cell Skin Cancer. V.2.2025. Available at https://www.nccn.org/professionals/physician_gls/pdf/nmsc.pdf. Last accessed February 12, 2025.
104. Tierney EP, Hanke CW. Cost effectiveness of Mohs micrographic surgery: review of the literature. J Drugs Dermatol. 2009;8(10): 914-922.
105. Fink-Puches R, Soyer HP, Hofer A, Kerl H, Wolf P. Long-term follow-up and histological changes of superficial nonmelanoma skin cancers treated with topical delta-aminolevulinic acid photodynamic therapy. Arch Dermatol. 1998;134(7):821-826.
106. Marmur ES, Schmults CD, Goldberg DJ. A review of laser and photodynamic therapy for the treatment of nonmelanoma skin cancer. Dermatol Surg. 2004;30(2 pt. 2):264-271.
107. Robinson JK. Follow-up and prevention (basal cell). In: Miller SJ, Maloney ME (eds). Cutaneous Oncology Pathophysiology, Diagnosis, and Management. Malden, MA: Wiley-Blackwell; 1998: 695-698.
108. Bain J. More than One? Available at https://www.skincancer.org/prevention/are-you-at-risk/more-than-one. Last accessed February 12, 2025.
109. Marghoob AA, Slade J, Salopek TG, Kopf AW, Bart RS, Rigel DS. Basal cell and squamous cell carcinomas are important risk factors for cutaneous malignant melanoma: screening implications. Cancer. 1995;75(2 suppl):707-714.
110. Shin DM, Maloney ME, Lippman SM. Follow-up and prevention (squamous cell carcinoma). In: Miller SJ, Maloney ME (eds). Cutaneous Oncology Pathophysiology, Diagnosis, and Management. Malden, MA: Wiley-Blackwell; 1998.
111. Goldberg MS, Doucette JT, Lim HW, Spencer J, Carucci JA, Rigel DS. Risk factors for presumptive melanoma in skin cancer screening: American Academy of Dermatology National Melanoma/Skin Cancer Screening Program experience, 2001–2005. J Am Acad Dermatol. 2007;57(1):60-66.
112. Hsu MY, Meier F, Herlyn M. Melanoma development and progression: a conspiracy between tumor and host. Differentiation. 2002;70(9-10):522-536.
113. Cho E, Rosner BA, Colditz GA. Risk factors for melanoma by body site. Cancer Epidemiol Biomarkers Prev. 2005;14(5):1241-1244.
114. Caini S, Gandini S, Sera F, et al. Meta-analysis of risk factors for cutaneous melanoma according to anatomical site and clinico-pathological variant. Eur J Cancer. 2009;45(17):3054-3063.
115. Ivry GB, Ogle CA, Shim EK. Role of sun exposure in melanoma. Dermatol Surg. 2006;32(4):481-492.
116. National Cancer Institute. Common Moles, Dysplastic Nevi, and Risk of Melanoma. Available at https://www.cancer.gov/types/skin/moles-fact-sheet. Last accessed February 12, 2025.
117. Titus-Ernstoff L, Perry AE, Spencer SK, et al. Multiple primary melanoma: two-year results from a population-based study. Arch Dermatol. 2006;142(4):433-438.
118. Gandini S, Sera F, Cattaruzza MS, et al. Meta-analysis of risk factors for cutaneous melanoma: I. Common and atypical naevi. Eur J Cancer. 2005;41(1):28-44.
119. National Cancer Institute Surveillance Epidemiology and End Results Program. Contents of the SEER Cancer Statistics Review, 1975–2012. Age Distribution at Diagnosis. Available at https://seer.cancer.gov/archive/csr/1975_2012/results_merged/topic_age_dist.pdf. Last accessed February 12, 2025.
120. McKenna JK, Florell SR, Goldman GD, Bowen GM. Lentigo maligna/lentigo maligna melanoma: current state of diagnosis and treatment. Dermatol Surg. 2006;32(4):493-504.
121. Brady MS, Oliveria SA, Christos PJ, et al. Patterns of detection in patients with cutaneous melanoma. Cancer. 2000;89(2):342-347.
122. Terushkin V, Halpern AC. Melanoma early detection. Hematol Oncol Clin N Am. 2009;23(3):481-500.
123. Chamberlain AJ, Fritschi L, Kelly JW. Nodular melanoma: patients' perceptions of presenting features and implications for early detection. J Am Acad Dermatol. 2003;48(5):694-701.
124. Friedman RJ, Rigel DS, Kopf AW. Early detection of malignant melanoma: the role of the physician examination and self-examination of the skin. CA Cancer J Clin. 1985;35(3):130-151.
125. Melanoma Research Foundation. What Melanoma Looks Like. Available at https://melanoma.org/melanoma-education/what-melanoma-looks-like/. Last accessed February 12, 2025.
126. Grin CM, Kopf AW, Welkovich B, Bart RS, Levenstein MJ. Accuracy in the clinical diagnosis of malignant melanoma. Arch Dermatol. 1990;126(6):763-766.
127. Shoo BA, Kashani-Sabet M. Melanoma arising in African-, Asian-, Latino-and Native-American populations. Semin Cutan Med Surg. 2009;28(2):96-102.
128. Cormier JN, Xing Y, Ding M, et al. Ethnic differences among patients with cutaneous melanoma. Arch Intern Med. 2006;166(17):1907-1914.
129. Bergfelt L, Newell GR, Sider JG, Kripke ML. Incidence and anatomic distribution of cutaneous melanoma among United States Hispanics. J Surg Oncol. 1989;40(4):222-226.
130. National Cancer Institute. Intraocular (Uveal) Melanoma Treatment (PDQ). Available at https://www.cancer.gov/types/eye/hp/intraocular-melanoma-treatment-pdq. Last accessed February 12, 2025.
131. Breslow A. Thickness, cross-sectional areas and depth of invasion in the prognosis of cutaneous melanoma. Ann Surg. 1970;172(5):902-908.
132. National Comprehensive Cancer Network. Clinical Practice Guidelines in Oncology: Cutaneous Melanoma. V.2.2025. Available at https:/www.nccn.org/professionals/physician_gls/pdf/cutaneous_melanoma.pdf. Last accessed February 12, 2025.
133. Jost LM, Jelic S, Purkalne G, ESMO Guidelines Task Force. ESMO minimum clinical recommendations for diagnosis, treatment and follow-up of cutaneous malignant melanoma. Ann Oncol. 2005;16(suppl 1):i66-i68.
134. Skin Cancer Foundation. After a Transplant: New Dangers. Available at https://www.skincancer.org/blog/after-a-transplant-new-dangers/. Last accessed February 12, 2025.
135. Balch CM, Soong SJ, Atkins MB, et al. An evidence-based staging system for cutaneous melanoma. CA Cancer J Clin. 2004;54(3):131-149.
136. Schmalbach CE, Bradford CR. Is sentinel lymph node biopsy the standard of care for cutaneous head and neck melanoma? Laryngoscope. 2015;125(1):153-160.
137. Phan GQ, Messina JL, Sondak VK, Zager JS. Sentinel lymph node biopsy for melanoma: indications and rationale. Cancer Control. 2009;16(3):234-239.
138. Larsen AK, Jensen MB, Krag C. Long-term survival after metastatic childhood melanoma. Plast Reconstr Surg Glob Open. 2014;2(6):e163.
139. Sladden MJ, Balch C, Barzilai DA, et al. Surgical excision margins for primary cutaneous melanoma. Cochrane Database Syst Rev. 2009;(4):CD004835.
140. Kavanagh D, Hill AD, Djikstra B, Kennelly R, McDermott EM, O'Higgins NJ. Adjuvant therapies in the treatment of stage II and III malignant melanoma. Surgeon. 2005;3(4):245-256.
142. Anaya DA, Xing Y, Feng L, et al. Adjuvant high-dose inferferon for cutaneous melanoma is most beneficial for patients with early stage III disease. Cancer. 2008;112(9):2030-2037.
143. Mocellin S, Pasquali S, Rossi CR, Nitti D. Interferon alpha adjuvant therapy in patients with high-risk melanoma: a systematic review and meta-analysis. J Natl Cancer Inst. 2010;102(7):493-501.
144. Ascierto PA, Scala S, Ottaiano A, et al. Adjuvant treatment of malignant melanoma: where are we? Crit Rev Oncol Hematol. 2006;57(1):45-52.
145. Dixon S, Walters SJ, Turner L, Hancock BW. Quality of life and cost-effectiveness of interferon-alpha in malignant melanoma: results from randomised trial. Br J Cancer. 2006;94(4):492-498.
146. Tarhini AA, Agarwala SS. Novel agents in development for the treatment of melanoma. Expert Opin Investig Drugs. 2005;14(7):885-892.
147. Tarhini AA, Agarwala SS. Interleukin-2 for the treatment of melanoma. Curr Opin Investig Drugs. 2005;6(12):1234-1239.
148. Atallah E, Flaherty L. Treatment of metastatic malignant melanoma. Curr Treat Options Oncol. 2005;6(3):185-193.
149. American Cancer Society. Treatment of Melanoma Skin Cancer by Stage. Available at https://www.cancer.org/cancer/melanoma-skin-cancer/treating/by-stage.html. Last accessed February 12, 2025.
150. U.S. Food and Drug Administration. FDA Approves Dabrafenib Plus Trametinib for Adjuvant Treatment of Melanoma with BRAF V600E or V600K Mutations. Available at https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-dabrafenib-plus-trametinib-adjuvant-treatment-melanoma-braf-v600e-or-v600k-mutations. Last accessed February 12, 2025.
151. U.S. Food and Drug Administration. Hematology/Oncology (Cancer) Approvals & Safety Notifications. Available at https://www.fda.gov/drugs/resources-information-approved-drugs/oncology-cancer-hematologic-malignancies-approval-notifications?t=529865. Last accessed February 12, 2025.
152. U.S. Food and Drug Administration. Ipilimumab. Available at https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/ 125377s087lbl.pdf. Last accessed February 12, 2025.
153. Hodi FS, O'Day SJ, McDermott DF, et al. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med. 2010;363(8):711-723.
154. LexiDrug. Available at http://online.lexi.com. Last accessed February 12, 2025.
155. U.S. Food and Drug Administration. Vemurafenib. Available at https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/202429s012lbl.pdf. Last accessed February 12, 2025.
156. Chapman PB, Hauschild A, Robert C, et al. Improved survival with vemurafenib in melanoma with BRAFV600E mutation. N Engl J Med. 2011;364(26):2507-2516.
157. Raedler LA. Keytruda (Pembrolizumab): First PD-1 inhibitor approved for previously treated unresectable or metastatic melanoma. Am Health Drug Benefits. 2015;8(Spec Feature):96-100.
158. Green AC, Williams GM, Logan V, Strutton GM. Reduced melanoma after regular sunscreen use: randomized trial follow-up. J Clin Oncol. 2011;29(3):257-263.
159. McMasters KM, Wong SL, Edwards MJ, et al. Factors that predict the presence of sentinel lymph node metastasis in patients with melanoma. Surgery. 2001;130(2):151-156.
160. Lens MB, Dawes M, Newton-Bishop JA, Goodacre T. Tumour thickness as a predictor of occult lymph node metastases in patients with stage I and II melanoma undergoing sentinel lymph node biopsy. Br J Surg. 2002;89(10):1223-1227.
161. Morton DL, Thompson JF, Cochran AJ, et al. Sentinel-node biopsy or nodal observation in melanoma. N Engl J Med. 2006;355(13):1307-1317.
162. Wong SL, Morton DL, Thompson JF, et al. Melanoma patients with positive sentinel nodes who did not undergo completion lymphadenectomy: a multi-institutional study. Ann Surg Oncol. 2006;13(6):809-816.
163. Wong SL, Faries MB, Kennedy EB, et al. Sentinel lymph node biopsy and management of regional lymph nodes in melanoma: American Society of Clinical Oncology and Society of Surgical Oncology clinical practice guideline update. J Clin Oncol. 2018;36(4):399-413.
164. Scott JD, McKinley BP, Bishop A, Trocha SD. Treatment and outcomes of melanoma with a Breslow's depth greater than or equal to one millimeter in a regional teaching hospital. Am Surg. 2005;71(3):198-201.
165. Cormier JN, Xing Y, Ding M, et al. Population-based assessment of surgical treatment trends for patients with melanoma in the era of sentinel lymph node biopsy. J Clin Oncol. 2005;23(25):6054-6062.
166. Bilimoria KY, Balch CM, Bentrem DJ, et al. Complete lymph node dissection for sentinel node-positive melanoma: assessment of practice patterns in the United States. Ann Surg Oncol. 2008;15(6):1566-1576.
167. National Cancer Institute Surveillance, Epidemiology, and End Results Program. Cancer Stat Facts: Melanoma of the Skin. Available at https://seer.cancer.gov/statfacts/html/melan.html. Last accessed February 12, 2025.
168. LeBlanc WG, Vidal L, Kirsner RS et al. Reported skin cancer screening of U.S. adult workers. J Am Acad Dermatol. 2008;59(1): 55-63.
169. Lakhani NA, Saraiya M, Thompson TD, King SC, Guy GP Jr. Total body skin examination for skin cancer screening among U.S. adults from 2000 to 2010. Prev Med. 2014;61:75-80.
170. U.S. Preventive Services Task Force. Screening for skin cancer: U.S. Preventive Services Task Force recommendation statement. JAMA. 2016;316(4):429-435.
171. Sanchez G, Nova J, Rodriguez-Hernandez A, et al. Sun protection for preventing basal cell and squamous cell skin cancers. Cochrane Database Syst Rev. 2016;7.
172. National Cancer Institute. Skin Cancer (Including Melanoma). Available at https://www.cancer.gov/types/skin/hp. Last accessed February 12, 2025.
173. American Academy of Family Physicians. AAFP Policy Action: Summary of Recommendations for Clinical Preventive Services, 2017. Available at https://www.aafp.org/dam/AAFP/documents/patient_care/clinical_recommendations/cps-recommendations.pdf. Last accessed February 12, 2025.
174. Skin Cancer Foundation. Basal Cell Carcinoma Warning Signs: Early Detection Best Practices. Available at https://www.skincancer.org/skin-cancer-information/basal-cell-carcinoma/bcc-warning-signs-images. Last accessed February 12, 2025.
175. Watts CG, Drummond M, Goumas C, et al. Sunscreen use and melanoma risk among young Australian adults. JAMA Dermatol. 2018;154(9):1001-1009.
176. Wernli KJ, Henrikson NB, Morrison CC, Nguyen M, Pocobelli G, Whitlock EP. Screening for Skin Cancer in Adults: An Updated Systematic Evidence Review for the U.S. Preventive Services Task Force. Rockville, MD: Agency for Healthcare Research and Quality; 2016.
177. American Academy of Dermatology. Skin Cancer Screening Program. Available at https://www.aad.org/public/public-health/skin-cancer-screenings. Last accessed February 13, 2025.
178. American Cancer Society. Skin Cancer Prevention and Early Detection. Available at https://www.cancer.org/cancer/skin-cancer/prevention-and-early-detection.html. Last accessed February 12, 2025.
179. Kantor J, Kantor DE. Routine dermatologist-performed full-body skin examination and early melanoma detection. Arch Dermatol. 2009;145(8):873-876.
180. Aitken JF, Elwood M, Baade PD, Youl P, English D. Clinical whole-body skin examination reduces the incidence of thick melanomas. Int J Cancer. 2010;126(2):450-458.
181. Geller AC, Miller DR, Swetter SM, Demierre MF, Gilchrest BA. A call for the development and implementation of a targeted national melanoma screening program. Arch Dermatol. 2006;142(4):504-507.
182. U.S. Preventive Services Task Force. Behavioral counseling to prevent skin cancer: U.S. Preventive Services Task Force recommendation statement. JAMA. 2018; 319(11):1134-1142.
183. Cancer Trends Progress Report. Prevention. UV Exposure and Sun Protective Practices. Available at https://www.progressreport.cancer.gov/prevention/sun_protection. Last accessed February 12, 2025.
184. Centers for Disease Control and Prevention. Skin Cancer. Available at https://www.cdc.gov/cancer/skin. Last accessed February 12, 2025.
185. Skin Cancer Foundation. Prevention Guidelines. Available at https://www.skincancer.org/skin-cancer-prevention/. Last accessed February 12, 2025.
186. National Cancer Institute. Health Information National Trends Survey (HINTS): Skin Protection. Available at https://hints.cancer.gov/docs/Briefs/HINTS_Brief_6_051607.pdf. Last accessed February 12, 2025.
187. Wheless L, Ruczinski I, Alani RM, et al. The association between skin characteristics and skin cancer prevention behaviors. Cancer Epidemiol Biomarkers Prev. 2009;18(10):2613-2619.
188. Cancer Trends Progress Report. Sunburn. Available at https://progressreport.cancer.gov/prevention/sunburn. Last accessed February 12, 2025.
189. Holman DM, Ding H, Guy GP Jr, et al. Prevalence of sun protection use and sunburn and association of demographic behavioral characteristics with sunburn among U.S. adults. JAMA Dermatol. 2018;154(5):561-568.
190. Dennis LK, Beane Freeman LE, VanBeek MJ. Sunscreen use and the risk for melanoma: a quantitative review. Ann Intern Med. 2003;139(12):966-978.
191. Autier P, Doré JF, Schifflers E, et al. Melanoma and use of sunscreens: an EORTC case-control study in Germany, Belgium and France: the EORTC melanoma cooperative group. Int J Cancer. 1995;61(6):749-755.
192. Green A, Williams G, Neale R, et al. Daily sunscreen application and beta carotene supplementation in prevention of basal-cell and squamous-cell carcinomas of the skin: a randomised controlled trial. Lancet. 1999;354(9180):723-729.
193. Dupuy A, Dunant A, Grob JJ, Réseau d'Epidémiologie en Dermatologie. Randomized controlled trial testing the impact of high-protection sunscreens on sun-exposure behavior. Arch Dermatol. 2005;141(8):950-956.
194. Wright MW, Wright ST, Wagner RF. Mechanisms of sunscreen failure. J Am Acad Dermatol. 2001;44(5):781-784.
195. Wesson KM, Silverberg NB. Sun protection education in the United States: what we know and what needs to be taught. Cutis. 2003;71(1):71-74, 77.
196. Geller AC, Brooks DR, Colditz GA, Koh HK, Frazier AL. Sun protection practices among offspring of women with personal or family history of skin cancer. Pediatrics. 2006;117(4):e688-e694.
197. Dadlani C, Orlow SJ. Planning for a brighter future: a review of sun protection and barriers to behavioral change in children and adolescents. Dermatol Online J. 2008;14(9):1.
198. Stern RS, Weinstein MC, Baker SG. Risk reduction for nonmelanoma skin cancer with childhood sunscreen use. Arch Dermatol. 1986;122(5):537-545.
199. National Cancer Institute. Health Information National Trends Survey (HINTS). Available at https://hints.cancer.gov/view-questions-topics/all-hints-questions.aspx. Last accessed February 13, 2025.
200. Eide MJ, Tuthill JM, Krajenta R, et al. Validation of claims algorithms to identify nonmelanoma skin cancer. J Invest Dermitol. 2012;132(8):2005-2009.
201. Muzic JG, Schmitt AR, Wright AC. Incidence and trends of basal cell carcinoma and cutaneous squamous cell carcinoma. Mayo Clinic Proceedings. 2017;92(6):890-898.
202. Cronin KA, Lake AJ, Scott S, et al. Annual report to the nation on the status of cancer, part I: national cancer statistics. Cancer. 2018;124(13):2785-2800.
203. REF D: Arnold M, de Vries E, Whiteman DC, et al. Global burden of cutaneous melanoma attributable to ultraviolet radiation in 2012. Int J Cancer. 2018;143(6):1305-1314.
204. Harvey VM, Patel H, Sandhu S, et al. Social determinants of racial and ethnic disparities in cutaneous melanoma outcomes. Cancer Control. 2014;21(4):343-349.
205. Sharma D, Friedman AJ, Redbord KP. Need for improved skin cancer surveillance in pediatric cancer survivors. Am J Clin Dermatol. 2017;18(2):165-168.
206. Willingham V. Sunlamps and Tanning Beds Get FDA Warning. Available at https://www.cnn.com/2014/05/29/health/tanning-sunlamps-labeling-fda. Last accessed February 13, 2025.
207. Berwick M, Begg CB, Fine JA, Roush GC, Barnhill RL. Screening for cutaneous melanoma by skin self-examination. J Natl Cancer Inst. 1996;88(1):17-23.
208. Lee KB, Weinstock MA, Risica PM. Components of a successful intervention for monthly skin self-examination for early detection of melanoma: the "Check It Out" trial. J Am Acad Dermatol. 2008;58(6):1006-1012.
209. Robinson JK, Turrisi R. Skills training to learn discrimination of ABCDE criteria by those at risk of developing melanoma. Arch Dermatol. 2006;142(4):447-452.
210. Robinson JK, Turrisi R, Stapleton J. Efficacy of a partner assistance intervention designed to increase skin self-examination performance. Arch Dermatol. 2007;143(1):37-41.
211. Committee on Health Literacy Board on Neuroscience and Behavioral Health. Health Literacy: A Prescription to End Confusion. Washington, DC: The National Academies Press; 2004.
212. Kirsch IS, Jungeblut A, Jenkins L, Kolstad A. Adult Literacy in America: A First Look at the Results of the National Adult Literacy Survey. 3rd ed. Washington, DC: National Center for Education Statistics, U.S. Department of Education; 2002.
213. U.S. Census Bureau. Selected Social Characteristics in the United States: 2023 American Community Survey 5-Year Estimates. Available at https://data.census.gov/table/ACSDP5Y2023.DP02?d=ACS 5-Year Estimates Data Profiles. Last accessed February 13, 2025.
214. Shepard S. Challenges in Cultural Diversity: Protect Your Patients and Yourself. Available at https://www.thedoctors.com/articles/challenges-of-cultural-diversity-in-healthcare-protect-your-patients-and-yourself. Last accessed February 13, 2025.
215. Karliner LS, Napoles-Springer AM, Schillinger D, Bibbins-Domingo K, Pérez-Stable EJ. Identification of limited English proficient patients in clinical care. J Gen Intern Med. 2008;23(10):1555-1560.
216. Sevilla Mátir JF, Willis DR. Using bilingual staff members as interpreters. Fam Pract Manag. 2004;11(7):34-36.
217. Ngo-Metzger Q, Massagli MP, Clarridge BR, et al. Linguistic and cultural barriers to care: perspectives of Chinese and Vietnamese immigrants. J Gen Intern Med. 2003;18(1):44-52.
218. Flores G. Language barriers to health care in the United States. N Engl J Med. 2006;355(3):229-231.
219. Flores G. The impact of medical interpreter services on the quality of health care: a systematic review. Med Care Res Rev. 2005;62(3):255-299.
220. Karliner LS, Jacobs EA, Chen AH, Mutha S. Do professional interpreters improve clinical care for patients with limited English proficiency? A systematic review of the literature. Health Serv Res. 2007;42(2):727-754.
221. Hwa-Froelich DA, Westby CE. Considerations when working with interpreters. Commun Disord Quart. 2003;24(2):78-85.
222. Zeitouni NC, Bhatia N, Ceilley RI, et al. Photodynamic therapy with 5-aminolevulinic acid 10% gel and red light for the treatment of actinic keratosis, nonmelanoma skin cancers, and acne: current evidence and best practices. J Clin Aesthet Dermatol. 2021;14(10):E53-E65.
223. Bichakjian CK, Schwartz JL, Wang TS, Hall JM, Johnson TM, Biermann JS. Melanoma information on the Internet: often incomplete-a public health opportunity? J Clin Oncol. 2002;20(1):134-141.
224. Pagoto S, Hillhouse J, Heckman CJ, et al. Society of Behavioral Medicine (SBM) position statement: ban indoor tanning for minors. Transl Behav Med. 2014;4(1):124-126.
225. American Academy of Dermatology. Amended Position Statement on Indoor Tanning. Available at https://www.aad.org/forms/policies/uploads/ps/ps%20-%20indoor%20tanning.pdf. Last accessed February 11, 2025.
226. American Academy of Pediatrics Council on Environmental Health and Section on Dermatology. Policy statement: ultraviolet radiation: a hazard to children and adolescents. Pediatrics. 2011;104(2):328.
227. Wu S, Han J, Laden F, Qureshi AA. Long-term ultraviolet flux, other potential risk factors, and skin cancer risk: a cohort study. Cancer Epidemiol Biomar Prev. 2014;23(6):1080-1089.
228. Yanofsky VR, Mercer SE, Phelps RG. Histopathological variants of cutaneous squamous cell carcinoma: a review. J Skin Cancer. 2011;210813:1-13.
229. Karisa PS, Morgan FC, Califano JA, Schmults CD. Comparison of tumor classifications for cutaneous squamous cell carcinoma of the head and neck in the 7th vs 8th edition of the AJCC Cancer Staging Manual. JAMA Dermatol. 2018;154(2):175-181.
230. Stevenson MM. Cutaneous Carcinoma of the Head and Neck Staging. Available at https://emedicine.medscape.com/article/2007181-overview. Last accessed February 12, 2025.
231. Keohane SG, Proby CM, Newlands C, et al. The new 8th edition of TNM staging and its implications for skin cancer: a review by the British Association of Dermatologists and the Royal College of Pathologists, U.K. Br J Dermatol. 2018;179(4):824-828.
232. National Cancer Institute. Skin Cancer Treatment (PDQ). Available at https://www.cancer.gov/types/skin/hp/skin-treatment-pdq. Last accessed February 12, 2025.
233. Morton CA. A synthesis of the world's guidelines on photodynamic therapy for non-melanoma skin cancer. G Ital Dermatol Venereol. 2018;153(6):783-792.
234. Hehlgans S, Booms P, Gullulu O, et al. Radiation sensitization of basal cell and head and neck squamous cell carcinoma by the Hedgehog pathway inhibitor vismodegib. Int J Mol Sci. 2018;19(9):2485.
235. American Cancer Society. Risk Factors for Melanoma Skin Cancer. Available at https://www.cancer.org/cancer/melanoma-skin-cancer/causes-risks-prevention/risk-factors.html. Last accessed February 12, 2025.
236. Skin Cancer Foundation. Types of Melanoma. Available at https://www.skincancer.org/skin-cancer-information/melanoma/types-of-melanoma. Last accessed February 12, 2025.
237. Aviles-Izquierdo JA, Molina-Lopez I, Rodriguez-Lomba E. Who detects melanoma? Impact of detection patterns on characteristics and prognosis of patients with melanoma. J Am Acad Dermatol. 2016;75(5):967-974.
238. Ross MI, Balch CM. Excision margins of melanoma make a difference: new data support an old paradigm. Ann Surg Oncol. 2016;23(4):1053-1056.
239. McMasters KM, Egger ME, Edwards MJ, et al. Final results of the sunbelt melanoma trial: a multi-institutional prospective randomized phase III study evaluating the role of adjuvant high-dose interferon alfa-2b and completion lymph node dissection for patients staged by sentinel lymph node biopsy. J Clin Oncol. 2016;34(1):1079-1086.
240. American Society of Clinical Oncology. Sentinel Lymph Node Biopsy for Melanoma. Available at https://www.asco.org/guidelines/GUIDELINEASCO9316. Last accessed February 12, 2025.
241. National Cancer Institute. HINTS Briefs. Available at https://hints.cancer.gov/docs/Briefs/HINTS_Brief_13.pdf. Last accessed February 12, 2025.
242. Skin Cancer Foundation. Sun-Protective Clothing. Available at https://www.skincancer.org/skin-cancer-prevention/sun-protection/sun-protective-clothing. Last accessed February 12, 2025.
243. U.S. Food and Drug Administration. FDA Approves Atezolizumab for BRAFV600 Unresectable or Metastatic Melanoma. Available at https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-atezolizumab-braf-v600-unresectable-or-metastatic-melanoma. Last accessed February 12, 2025.
244. U.S. Food and Drug Administration. FDA Approves Pembrolizumab for Adjuvant Treatment of Stage IIB or IIC Melanoma. Available at https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-pembrolizumab-adjuvant-treatment-stage-iib-or-iic-melanoma. Last accessed February 12, 2025.
245. U.S. National Library of Medicine. Safety and Efficacy of Pembrolizumab Compared to Placebo in Resected High-risk Stage II Melanoma (MK-3475-716/KEYNOTE-716). Available at https://clinicaltrials.gov/ct2/show/NCT03553836. Last accessed February 12, 2025.
246. U.S. Food and Drug Administration. FDA Grants Regular Approval to Nivolumab for Adjuvant Treatment of Melanoma. Available at https://www.fda.gov/drugs/resources-information-approved-drugs/fda-grants-regular-approval-nivolumab-adjuvant-treatment-melanoma. Last accessed February 12, 2025.
247. U.S. Food and Drug Administration. Cobimetinib: Approval Letter. Available at https://www.accessdata.fda.gov/drugsatfda_docs/nda/2015/206192Orig1s000Approv.pdf. Last accessed February 12, 2025.
1. Kim JYS, Kozlow JH, Mittal B, et al. Guidelines of care for the management of basal cell carcinoma. J Am Acad Dermatol. 2018;78(3):540-559. Available at https://www.jaad.org/article/S0190-9622(17)32529-X/fulltext. Last accessed February 21, 2025.
2. Wong SL, Faries MB, Kennedy EB, et al. Sentinel lymph node biopsy and management of regional lymph nodes in melanoma: American Society of Clinical Oncology and Society of Surgical Oncology clinical practice guideline update. J Clin Oncol. 2018;36(4):399-413. Available at http://ascopubs.org/doi/10.1200/JCO.2017.75.7724. Last accessed February 21, 2025.
3. U.S. Preventive Services Task Force, Grossman DC, Curry SJ, et al. Behavioral counseling to prevent skin cancer: U.S. Preventive Services Task Force recommendation statement. JAMA. 2018;319(11):1134-1142. Available at https://jamanetwork.com/journals/jama/fullarticle/2675556. Last accessed February 21, 2025.
Mention of commercial products does not indicate endorsement.