Burnout is a syndrome of emotional exhaustion, depersonalization, and reduced personal accomplishment. Levels of burnout are high among physicians, with even higher rates among physicians in training. High degrees of job dissatisfaction and stress precede burnout, making it incumbent on physicians to recognize stress early to help prevent burnout before it occurs. Preventing burnout is vital not only for the well-being and professional preservation of physicians but also for ensuring optimal patient outcomes. Several personal and professional lifestyle strategies can help physicians cope with stress, achieve better work-life balance, and become more engaged in their work.
This course is designed for all physicians in all settings, especially oncology, palliative care, mental health, and critical care.
The prevalence of burnout among physicians is higher than that among the general U.S. population. The purpose of this course is to provide information on personal and professional strategies to cope with stress and avoid burnout.
Upon completion of this course, you should be able to:
- Define burnout and its relationship to job dissatisfaction and stress.
- Identify the work environment and personal risk factors for burnout.
- Recognize the most common physical, psychological, and interpersonal/social signs and symptoms of stress and burnout and tools to measure burnout.
- Discuss the prevalence of burnout among physicians.
- Explain the primary causes of stress and burnout among physicians.
- Describe the effects of physician burnout on the quality of health care.
- Select personal and professional lifestyle changes to manage stress and prevent burnout.
Lori L. Alexander, MTPW, ELS, MWC, is President of Editorial Rx, Inc., which provides medical writing and editing services on a wide variety of clinical topics and in a range of media. A medical writer and editor for more than 30 years, Ms. Alexander has written for both professional and lay audiences, with a focus on continuing education materials, medical meeting coverage, and educational resources for patients. She is the Editor Emeritus of the American Medical Writers Association (AMWA) Journal, the peer-review journal representing the largest association of medical communicators in the United States. Ms. Alexander earned a Master’s degree in technical and professional writing, with a concentration in medical writing, at Northeastern University, Boston. She has also earned certification as a life sciences editor and as a medical writer.
Contributing faculty, Lori L. Alexander, MTPW, ELS, MWC, has disclosed no relevant financial relationship with any product manufacturer or service provider mentioned.
John M. Leonard, MD
John V. Jurica, MD, MPH
The division planners have disclosed no relevant financial relationship with any product manufacturer or service provider mentioned.
Sarah Campbell
The Director of Development and Academic Affairs has disclosed no relevant financial relationship with any product manufacturer or service provider mentioned.
The purpose of NetCE is to provide challenging curricula to assist healthcare professionals to raise their levels of expertise while fulfilling their continuing education requirements, thereby improving the quality of healthcare.
Our contributing faculty members have taken care to ensure that the information and recommendations are accurate and compatible with the standards generally accepted at the time of publication. The publisher disclaims any liability, loss or damage incurred as a consequence, directly or indirectly, of the use and application of any of the contents. Participants are cautioned about the potential risk of using limited knowledge when integrating new techniques into practice.
It is the policy of NetCE not to accept commercial support. Furthermore, commercial interests are prohibited from distributing or providing access to this activity to learners.
Supported browsers for Windows include Microsoft Internet Explorer 9.0 and up, Mozilla Firefox 3.0 and up, Opera 9.0 and up, and Google Chrome. Supported browsers for Macintosh include Safari, Mozilla Firefox 3.0 and up, Opera 9.0 and up, and Google Chrome. Other operating systems and browsers that include complete implementations of ECMAScript edition 3 and CSS 2.0 may work, but are not supported. Supported browsers must utilize the TLS encryption protocol v1.1 or v1.2 in order to connect to pages that require a secured HTTPS connection. TLS v1.0 is not supported.
The role of implicit biases on healthcare outcomes has become a concern, as there is some evidence that implicit biases contribute to health disparities, professionals' attitudes toward and interactions with patients, quality of care, diagnoses, and treatment decisions. This may produce differences in help-seeking, diagnoses, and ultimately treatments and interventions. Implicit biases may also unwittingly produce professional behaviors, attitudes, and interactions that reduce patients' trust and comfort with their provider, leading to earlier termination of visits and/or reduced adherence and follow-up. Disadvantaged groups are marginalized in the healthcare system and vulnerable on multiple levels; health professionals' implicit biases can further exacerbate these existing disadvantages.
Interventions or strategies designed to reduce implicit bias may be categorized as change-based or control-based. Change-based interventions focus on reducing or changing cognitive associations underlying implicit biases. These interventions might include challenging stereotypes. Conversely, control-based interventions involve reducing the effects of the implicit bias on the individual's behaviors. These strategies include increasing awareness of biased thoughts and responses. The two types of interventions are not mutually exclusive and may be used synergistically.
#41033: Burnout in Physicians
Work is a significant source of stress in all occupations. According to the American Institute of Stress, 83% of Americans report experiencing work-related stress, with as many as half saying they need help managing it [1]. A nationwide survey by the American Psychological Association (APA) reported in 2023 that 77% of employees have experienced work-related stress in the previous month [2]. Work-related stress that is left unaddressed has the potential to develop into burnout over a period of time. The costs of burnout are even higher than stress and affect not only the well-being of the individual but that of the individual's family, friends, and colleagues. Burnout among physicians and other healthcare professionals carries the additional consequence of negatively affecting the quality of patient care and health outcomes. This consequence is even greater, given the high rates of burnout among physicians, rates that are higher than among the general U.S. population.
This course provides an overview of burnout, addressing its development, characteristics, and measurement. The prevalence of burnout according to several variables is discussed, as are the most common causes of stress and burnout. The effect of burnout on patient outcomes is noted, and strategies to cope with stress and avoid burnout are described.
The term "burnout" originated in the 1940s as a word to describe the point at which a jet or rocket engine stops operating [3]. The word was first applied to humans in the 1970s by the psychiatrist Herbert Freudenberger, who used the term to describe the status of overworked volunteers in free mental health clinics [4]. He compared the loss of idealism in these volunteers to a building—once a vital structure—that had burned out, and he defined burnout as the "progressive loss of idealism, energy, and purpose experienced by people in the helping professions as a result of the condition of their work" [5].
The term burnout is used (perhaps overused) by many, and definitions have varied since the time the word was first applied to humans. The word has been used to describe a mild degree of unhappiness caused by stress, as well as any degree of distress, from fatigue to major depression [6]. In the early 1980s, social psychologist Christina Maslach and her colleagues began to explore the loss of emotional feeling and concern for clients among human services professionals. Since then, she has researched burnout extensively, becoming the leading authority on the topic and the author of the criterion standard tool to assess burnout, the Maslach Burnout Inventory (MBI) [7,8,9].
Maslach emphasizes that burnout is not a problem related to an individual [9]. Instead, her research indicates that burnout is a problem of the social environment in which people work and is a function of how people within that environment interact with one another and perform their jobs [9]. She notes that burnout is more likely when there is a "major mismatch between the nature of the job and the nature of the person who does the job" [9]. These mismatches are at the core of the development of burnout. The term burnout is now usually limited to mean burnout as described by Maslach: a syndrome of emotional exhaustion, depersonalization, and reduced personal accomplishment [6].
The World Health Organization (WHO) also now recognizes burnout as a "syndrome conceptualized as resulting from chronic workplace stress that has not been successfully managed" [119]. This definition, which appears in the 11th revision of the International Classification of Diseases (ICD-11), makes an important distinction from the definition of burnout from the ICD-11-CM, which did not list burnout as a syndrome, but rather a "state of vital exhaustion" [120].
Burnout can occur in any setting, and it has been studied most extensively in a wide range of occupations within the human services field, from healthcare professionals to teachers, police, and prison workers [6]. High levels of burnout among healthcare professionals have been well documented.
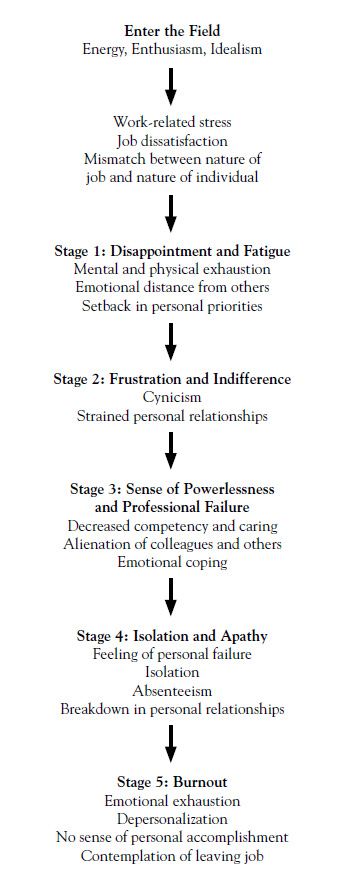
In general, when an individual first enters a chosen career, he or she is motivated. If the work environment is not supportive of the individual's efforts and concerns, the reality of the job and the individual's expectations begin to diverge and frustration and disappointment arise [6]. These feelings can lead to job dissatisfaction, resulting in decreased productivity, loss of confidence and enthusiasm, and behavior changes. If the situation is not addressed, stress accumulates and causes typical stress-related symptoms. These physical symptoms, when coupled with emotional emptiness, signify the first stage of burnout: mental and physical exhaustion [8]. Left untreated, burnout will continue through four more stages: indifference, feelings of failure as a professional, feelings of failure as a person, and emotional numbness (being "dead inside") (Figure 1) [8].
The specific factors within the work environment that lead to stress and subsequent burnout vary among occupations and among individuals within a single occupation. The root of burnout is in the work environment, but because not all individuals working in a single environment will experience burnout, personal risk factors must have a role in making an individual vulnerable. These personal risk factors include demographic variables and personality traits (Table 1) [6].
POTENTIAL RISK FACTORS FOR BURNOUT
| Dimension | Risk Factor | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Work environment |
| ||||||||||||
| Demographic variables |
| ||||||||||||
| Personality traits |
|
Burnout is more likely when an individual's experience (actual or perceived) does not match one or more situational factors in a work environment [9]. Among the mismatches that most commonly lead to burnout in any work environment are [9]:
Work overload: Limitations in terms of staff, time, and other resources
Lack of control: Unable to perform job functions the way an individual believes is the "right" way
Insufficient reward: Absence of acknowledgment of an individual's contributions in the work environment and lack of opportunities to advance
Absence of community: Poor working relationships, absence of adequate supervisory or peer support, poor leadership style
Lack of fairness: Inequality in workload, salary, or other signs of professional respect
Conflict in values: Disagreement between job requirements and an individual's personal principles
Demographic variables have been studied in relation to burnout, and several have been found to influence the risk of burnout, alone or in combination, including [6]:
Age
Sex
Family status
Educational status
Personality traits
Burnout is less prevalent among older individuals because they tend to be more stable and have a more balanced perspective on life [6]. In addition, the increased rate of burnout among younger individuals is a function of a "survival of the fittest" concept. Burnout usually occurs early in one's career (in the first one to five years), and many young, burned-out individuals leave the profession; as a result, the remaining individuals in an occupation are the "survivors" [6].
Across most work settings, levels of burnout have been somewhat consistent among men and women. One meta-analysis demonstrated similar overall rates of burnout among men and women, but there were differences between the sexes with regard to burnout components, with slightly higher levels of emotional exhaustion among women and somewhat higher levels of depersonalization among men [10]. Differences in burnout among male and female physicians will be discussed later in this course.
Family status also seems to play an important role in burnout; rates of burnout are higher among single workers and workers with no children than among married workers and those with children [6]. The emotional resources provided by a family are thought to be the reason for this difference.
In general, educational status seems to have an effect, with higher levels of burnout among workers with higher levels of education [6]. This difference could be the result of the expectations associated with advanced education and job choices [6]. In a study in which burnout was compared among physicians and the general population, an MD or DO degree was associated with a higher risk of burnout, whereas a Bachelor's degree, Master's degree, or doctoral degree (other than MD or DO) was associated with a lower risk [11].
Studies have also been done to explore the relationships between personality traits and the risk of burnout. Maslach noted that characteristics such as low self-esteem or lack of confidence, failure to recognize personal limits, need for approval, drive to overachieve, need for autonomy, impatience, intolerance, and empathy increased susceptibility to burnout [6]. Others have postulated that extreme conscientiousness, perfectionism, and self-giving (selflessness) also increase susceptibility, as does a type D personality (a joint tendency for negative emotions and social inhibition) [12,13,14]. Many of these personality traits are common among physicians; in fact, several are essential for success in this profession, which may explain, in part, the high levels of burnout among physicians.
Identifying the signs of stress and burnout is important to preserve the overall health and well-being of individuals. Burnout is associated with many signs and symptoms. For accurate identification, care should be taken to distinguish burnout from other conditions, such as stress, prolonged fatigue, and depression (Table 2) [6,15,16,17,18].
DISTINCTION BETWEEN BURNOUT AND CLINICAL ENTITIES WITH SIMILAR PRESENTATION
| Other Clinical Entity | Burnout | ||
|---|---|---|---|
| Result of prolonged stress | ||
| Associated with job-related factors | ||
| Related to specific factors in the work setting |
Stress can cause many of the same physical, psychological, and interpersonal/social symptoms as burnout. However, stress is distinct from burnout in that it is usually precipitated by isolated or situational instances, whereas burnout is the result of prolonged stress [6]. Prolonged fatigue often overlaps with burnout, but the precipitating factor differs for each; fatigue is usually associated with health-related causes, whereas burnout is caused by job-related factors [15,16].
Depression and burnout may have a similar clinical presentation, and signs of depression can be associated with burnout. However, depression is related to factors within every domain of an individual's life and is not limited to specific factors in the work setting [17,18]. Depression is more likely among individuals who have had a recent loss or a personal or family history of depression, but burnout is more likely if symptoms are worse in the work environment and if the individual works long hours and has no time for outside interests.
The most important distinction between burnout and all of these entities is that only burnout is characterized by the collective features of emotional exhaustion, depersonalization, and lack of accomplishment, as measured on the MBI.
The signs and symptoms of stress and burnout are multidimensional, with physical, psychological/psychiatric, and interpersonal/social manifestations (Table 3) [1,2,8,19,20]. As such, a multidisciplinary approach should be taken not only to confirm the presence of burnout but also to rule out other illnesses or conditions. In addition to the traditional medical history and physical examination, a social and occupational history should be obtained in an effort to identify potential stress factors and possible social consequences [8]. An evaluation of the type, course, and frequency of symptoms can help distinguish them as signs of burnout, and a drug history can help to identify potential substance abuse problems. The signs and symptoms of burnout discussed here are similar across work settings. Burnout among physicians is associated with these characteristics as well as some unique features, which will be described later.
SYMPTOMS ASSOCIATED WITH STRESS AND BURNOUT
| Dimension | Manifestation | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Physical |
| |||||||||||||||||
| Psychological |
| |||||||||||||||||
| Interpersonal/social |
|
The criterion standard for measuring burnout is the MBI, a self-assessment tool first published in 1981 by Maslach and Jackson [7]. The MBI was originally developed for the human services industry [121]. Since then, four additional versions have been developed, including a general survey, surveys for educators and students, and a medical personnel-specific survey [8]. The tool has been shown to be reliable, valid, and easy to administer and has been translated into several languages for use around the world. The MBI is often used in conjunction with other assessments to evaluate the relationship between burnout and organizational policies, productivity, and social support [7].
The MBI addresses the three defining aspects of burnout syndrome with 22 statements in three subscales [6]:
Emotional exhaustion: Nine statements to measure feelings of being emotionally overextended and exhausted by one's work
Depersonalization: Five statements to measure an unfeeling and impersonal response to the recipients of one's services, care treatment, or instruction
Personal accomplishment: Eight statements to measure feelings of competence and successful achievement in one's work
Each statement in the MBI expresses a particular feeling or attitude; for example, one statement in the depersonalization subscale is "I've become more callous toward people since I took this job" [6]. For each statement, the respondent indicates how frequently he or she experiences that feeling by using a fully anchored scale ranging from 0 (never) to 6 (every day). Higher scores on the emotional exhaustion and depersonalization subscales indicate higher degrees of burnout. A lower score on the personal accomplishment subscale corresponds to a lower degree of burnout. A separate score is determined for each subscale, and a scoring key provides threshold scores to indicate a low, average, or high degree of burnout on each subscale.
Because the length of the MBI may limit its use, researchers have explored the use of single-item measures from the instrument. Studies of healthcare professionals have shown that responses to one statement in the emotional exhaustion subscale ("I feel burned out from my work") and one statement in the depersonalization subscale ("I have become more callous toward people since I took this job") correlate well with the results of the full inventory [21,22]. More recently, a nonproprietary single-item measure has been shown to be a reliable substitute for the emotional exhaustion subscale of the MBI [23].
The use of tools to assess well-being or psychological status in conjunction with the full MBI can help professionals gain a better understanding of the sources of stress for individuals. The Mayo Clinic Physician Well-Being Index is often used in studies of burnout among physicians [24]. In addition, the General Health Questionnaire, developed by Goldberg, is designed to measure common mental health problems (domains of depression, anxiety, somatic symptoms, and social withdrawal) and was developed as a measure to identify individuals who are likely to have or be at risk for the development of psychiatric disorders [25].
Physicians certainly fall into the category of human services professionals and so are especially vulnerable to burnout [6]. The 2024 Survey of America's Physicians, conducted by the Physicians Foundation, found that 6 in 10 physicians reported often feeling burnout at work, a number which has remained consistent since increasing from 4 in 10 in 2018 [123,127]. Multiple factors have contributed to this number, including burnout related to the COVID-19 pandemic, as well as a trend in healthcare towards consolidating facilities, leaving physicians navigating change and often dealing with staff shortages [123,124,126]. In addition to the emotional strain of dealing with people who are sick or dying and who have extreme physical and/or emotional needs, features unique to medical practice and the evolving state of health care create additional stress for physicians [26]. Somewhat novel stressors contributing to burnout emerged at various points during the pandemic. These range from the initial uncertainty regarding COVID transmission, shortages of personal protective equipment, lack of effective treatments, and an overwhelming workload (in some settings) to later-stage factors, such as the politicization of social distancing, masking, and vaccination; incivility; and the multiple, frequent waves of disease [124]. Many physicians (49% overall, though markedly higher among surgeons) saw their incomes drop significantly early in the pandemic and many dealt with a reduction in staff (32%), while some shifted to working outside their area of expertise or had to adopt standards of care that were suboptimal [123,124].
As noted earlier, stress and job dissatisfaction play a role early in the development of burnout, and studies have confirmed that job or professional dissatisfaction is associated with burnout among physicians [27,28,29]. In 2023, the Survey of America's Physicians found that 71% of physicians believe financial gain to be the top priority of the hospitals they work for; many also believe that mergers and acquisitions have impacted patient outcomes negatively and will continue to do so [126]. These findings highlight the need to understand and address causes of stress and job dissatisfaction among physicians in order to prevent burnout.
Burnout has been studied among physicians in general, as well as across the span of their careers (medical students, fellows) and across specialties. The rates of burnout vary among these subgroups, but in general, the rates are higher than among workers in the general population and have increased over the past few years [11,30,31].
Since the early 2000s, many studies and surveys have been done to assess burnout in physicians, and the rates have ranged from 27% to 63%, with rates of 50% to 78% among medical students and residents [28,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,123,124]. These rates are somewhat consistent with the findings of more recent surveys of physicians in all specialties. One of these surveys, a 2014 study of nearly 7,000 physicians, showed an overall rate of burnout of 54% [30]. Another survey, reported on in the 2015 Medscape Lifestyle Report, represents the findings from nearly 20,000 physicians; the overall burnout rate was 46% [31]. Because burnout can be assessed and reported differently in each survey, it can be useful to look at the change over time in each. The rates in both surveys are higher than those previously reported by both authors: from 46% in 2011 to 54% in the 2014 study, and from 40% in 2013 to 46% in the 2015 report [30,31]. These rates reflect a much higher rate of burnout among physicians compared with the general U.S. population, which was reported to be 28% in 2014 [30]. The 2021 Physicians Foundation and AMA/Mayo Clinic surveys reported burnout rates of 61% and 62.8%, respectively [123,124].
The Mayo Clinic, which has been studying burnout rates for more than a decade, found that 2014 seemed to be a peak [125]. Burnout rates across nearly all specialties increased greatly that year compared to 2011, but in their 2017 survey, rates dropped precipitously and continued that trend in 2020. Six to nine months into the COVID-19 pandemic, the 2020 Mayo Clinic survey did not indicate that physician burnout had again increased. However, 12 to 15 months later, burnout in nearly all specialties increased precipitously.
As Maslach noted, the prevalence of burnout among physicians varies according to several factors, including age, sex, marital status, and career stage [6]. In addition, among physicians, the prevalence varies according to specialty area.
Age is a factor in burnout among physicians, with the lowest rate (35%) among physicians 34 years of age and younger [47]. The highest rates of burnout are found for physicians who are middle-age: 50% for physicians 45 to 54 years of age and 44% for physicians 35 to 44 years of age [128].
Specialty has an effect on the prevalence according to age. For example, in the Medscape survey, the overall burnout rate was 35% for physicians 34 years or younger, but rates were much higher among physicians in small specialties such as urology (54%), neurology (53%), and physical medicine and rehabilitation (52%) [31,128].
In a survey of family physicians and general internists, female physicians were nearly twice as likely as male physicians to report burnout (36% vs. 19%) [29]. Other studies have found differences in burnout according to sex, but not at the same magnitude. For example, Dyrbye et al. found burnout rates of 43% for female surgeons and 39% for male surgeons, and in the Medscape survey, the rates were 51% and 43% for female and male physicians, respectively [31,48]. The 2021 Physicians Foundation survey found that 69% of female physicians reported "often experience feeling of burnout," compared with 57% of male physicians [123]. As with physicians overall, the burnout rates among women have varied substantially according to specialty, with the highest rates for female physicians found in urology (67%), orthopedics (61%), critical care (61%), cardiology (60%), general surgery (59%), and emergency medicine (58%) [31]. Among residents, women are more likely than men to have burnout according to scores on the emotional exhaustion and personal achievement subscales [29].
In keeping with Maslach's theory that burnout usually occurs within the first five years of an individual's career, burnout rates are higher among medical students and residents than among physicians. In one study, the odds of burnout were higher for residents and fellows than for medical students and early-career physicians, and all three of these groups were significantly more likely to be burned out than college graduates of similar ages in other careers [49]. Similarly, a systematic review showed that residents in surgical specialties were more likely to be burned out than attending surgeons [50]. At the other end of the spectrum, the burnout rate is low among internal medicine residency program directors, with a rate of overall burnout of approximately 29% in one study [38]. In a comparison of burnout among physicians in early, middle, or late career (10 years or less, 11 to 20 years, and 21 years or more, respectively), the rate for depersonalization was highest among middle-career physicians [51]. The high rates of burnout among physicians in training are of concern because when burnout develops early during training, it tends to persist throughout residency [35].
Over the years, the rate of burnout among physicians has varied across specialties, with the highest rates reported among so-called high-stress specialties, such as critical care, emergency medicine, and oncology, as well as among physicians on the frontline of care, such as family practice and internal medicine [11]. The rates found in the 2019 Medscape report are somewhat consistent with this trend, with critical care, neurology, family medicine, obstetrics/gynecology, and internal medicine being the specialties with the highest rates of burnout [47]. The 2021 AMA/Mayo Clinic survey noted that burnout greatly increased among physicians practicing in emergency medicine, critical care medicine, hospital medicine, and infectious disease during the COVID-19 pandemic, and the 2024 Medscape report continues to bear this out (Table 4) [124,129]. The rate of burnout in emergency medicine increased from a reported 48% to 63%, while subspecialities of internal medicine such as pulmonology and oncology increased from 39% to 50% and 39% to 53%, respectively. Obstetrics/gynecology rose from 45% to 53% between 2019 and 2025. While some specialties, such as urology, neurology, and physical medicine and rehabilitation, have shown slightly lower rates of burnout, the general trend across specialties shows an increase both during and after the COVID-19 pandemic [129].
BURNOUT RATE ACCORDING TO PHYSICIAN SPECIALTY, 2024
| Physician Specialty | Burnout Rate |
|---|---|
| Urology | 49% |
| Neurology | 44% |
| Physical medicine and rehabilitation | 46% |
| Internal medicine | 51% |
| Emergency medicine | 63% |
| Family medicine | 51% |
| Diabetes and endocrinology | 44% |
| Surgery, general | 45% |
| Gastroenterology | 50% |
| Obstetrics/gynecology (women's health) | 53% |
| Radiology | 51% |
| Critical care | 45% |
| Cardiology | 47% |
| Anesthesiology | 50% |
| Pediatrics | 51% |
| Oncology | 53% |
| Psychiatry | 39% |
| Pulmonary medicine | 50% |
| Dermatology | 46% |
| Orthopedics | 44% |
| Otolaryngology | 43% |
| Plastic surgery | 37% |
| Ophthalmology | 39% |
| Pathology | 41% |
| Nephrology | 46% |
The 2025 Medscape report also includes information on the degree of burnout, noting the percentage of respondents who reported severe burnout (a score of 5 on a scale of 1 to 5, with 5 defined as "so severe that I'm thinking of leaving medicine"). An estimated 14% of men and 16% of women surveyed reported this most severe type of burnout. A higher percentage of physicians were in the middle range (rating a 3), 38% in men and 35% in women. Perhaps more concerningly, however, was the percentage of physicians who have reported experiencing burnout for more than two years, which increased in the 2025 report to 42% [129].
The job-related factors contributing to burnout among physicians are similar to those in non-healthcare settings. The most commonly reported causes of stress, job dissatisfaction, and burnout—across career stages and specialties—are work overload, inadequate work-life balance, and lack of control over one's work, causes that are in line with the work environment factors described by Maslach [6,11,29,38,40,45,52]. In addition, physicians are challenged by many stressors unique to the practice of medicine, such as practice demands, evolving health policy, difficult or complex patients, and an inability to keep up with research (Table 5) [26,31,53]. Information technology has changed physicians' work environments, and this, too, is a factor contributing to burnout. Again, the importance of these causative factors varies across specialties.
MOST COMMON CAUSES OF BURNOUT AMONG PHYSICIANS
|
Nearly half of physicians report that their job is "extremely stressful," and 80% say they feel "overextended," "overworked," or "at full capacity" [37,53]. Physicians also note that they have "too many patient appointments," leading to increased time pressure during visits, which has been strongly associated with lower rates of satisfaction and higher rates of burnout [29,54]. Long hours, many of which are spent on nonclinical tasks, and unsatisfactory work-life balance are the key factors in feeling stressed or overextended. Physicians work an average of 51 to 63 hours per week, or 11 to 23 more hours per week than the mean for the general population [30,34,44,48,53,55].
Approximately 60% of physicians have also noted time pressure associated with electronic documentation [56]. Physicians have reported that they spend an average of 9 to 11 hours per week on administrative (nonclinical) duties, with approximately 38% saying they work 11 hours or more each week on such duties [53,57]. Thus, tasks such as billing, obtaining insurance approvals, financial and personnel management, and negotiating contracts take up 14% to 23% of their work time [53,57]. An excess of "bureaucratic" tasks was the highest ranked cause of burnout in the Medscape Lifestyle Reports, and long hours at work was the second leading cause [31,47]. The time spent on administrative tasks takes away from time forming relationships with patients, the most satisfying factor about medical practice according to approximately 79% of physicians [53].
Long hours at work create conflicts between responsibilities at work and at home, and rates of work-life conflicts among physicians have been reported to range from 41% to 62%, and only 33% to 48% of physicians are satisfied with their work-life balance [11,34,40,47,48,58]. Both long hours and work-life conflicts have been found to be significantly associated with burnout [34,46,48,50,51]. Physicians' satisfaction with work-life balance has decreased since 2011 and is significantly lower than the rate among the general population (61% vs. 36%) [30]. Pooled multivariate analysis with adjustments for age, sex, relationship status, and hours worked per week showed that, compared with the general population, physicians had an increased risk of burnout and a decreased likelihood of being satisfied with work-life balance [30].
The era of information technology in medical practice, most notably electronic health records (EHRs) and computerized physician order entry (CPOE), began in the 1990s, and the technologies have been slow in becoming embraced by the medical community because they are challenging and time-consuming to learn [37]. Approximately 85% of physicians currently use these technologies, and about 60% think that EHRs have improved the quality of care [37]. However, the technology has been slow to improve efficiency of care. Surveys have shown that approximately 43% to 75% of physicians think that EHRs decrease efficiency and 47% to 66% of physicians think that using EHRs detracts from patient interaction [37,53,59]. One study showed that physicians who used EHRs spent slightly more time on administrative tasks than physicians who used paper records (17% of work time vs. 15% of work time) [57]. In another study, emergency department physicians spent a mean of 43% of their time on data entry, a significant difference from the time they spent on direct patient care (28%) [60]. In general, physicians are dissatisfied with the amount of time they spend using electronic documentation systems, and stress levels increase and satisfaction levels decrease with increasing use of EHRs [56,61,62]. Physicians who use EHRs and CPOE are also at higher risk for burnout, and "increased computerization of practice" was the fourth most common cause of burnout in the Medscape Lifestyle Reports [31,61,47]. As more physicians become comfortable with using electronic systems, their satisfaction may improve.
Physicians' autonomy is defined as the ability to determine how they work and decide how much time to spend with patients, what kinds of tests to perform, and what treatments to plan [63]. Autonomy has been reported to be the most important determinant of career satisfaction, yet it appears to be slowly eroding [64,65]. Approximately 50% to 69% of physicians say their clinical autonomy is sometimes or often limited and their decisions are sometimes or often compromised [53,56]. Physicians report being frustrated with decision-making by third parties (insurance companies and government agencies) and restrictions imposed by formularies or guidelines [66]. This loss of physician autonomy has been found to be significantly associated with burnout; lack of clinical and administrative autonomy were both significantly correlated with burnout in emergency physicians, and low control over work was strongly associated with dissatisfaction and burnout among primary care physicians [29,54,66,67,68]. Subjective factors, such as a perception of lack of autonomy, have had a stronger correlation with burnout than objective factors [39].
Many other factors have been noted to be risk factors for physician burnout. According to Maslach, insufficient reward for one's contributions is a risk factor for burnout, and this factor has been shown in studies of physicians. Insufficient income was fifth most commonly selected cause of burnout in the 2019 Medscape Lifestyle Report, and feeling unappreciated was a substantial contributor to burnout in a study of residents [47]. Poor working relationships with colleagues, analogous to Maslach's absence of community, has been reported to be a risk factor for burnout among critical care physicians and nurses [19]. In contrast, good working relationships with other physicians and staff have been associated with a greater likelihood of job satisfaction [54,69].
A factor unique to physicians was found in a 2010 study of U.S. surgeons, in which being sued for malpractice in the last 24 months was strongly associated with burnout [70]. Also unique to physicians is health policy; the impact of the Affordable Care Act was the fifth most common cause of burnout in the 2015 Medscape Lifestyle Report [31]. As many as half of physicians say their work environment is chaotic, and this factor has also been significantly associated with burnout [29,37,54].
Several studies have focused on the relationship between burnout and a variety of factors. The psychological factors of most concern for physicians are alcohol abuse/dependence, depression, and suicidal ideation (Table 6) [43,71,72,73,74]. Patient care is also a primary concern, as the symptoms of burnout have been linked to suboptimal patient outcomes.
PREVALENCE OF MENTAL HEALTH FACTORS IN PHYSICIANS AND MEDICAL STUDENTS/RESIDENTS VS. THE GENERAL POPULATION
| Factors | Physicians | Medical Students (MS) or Residents/Fellows (R/F) | General Population |
|---|---|---|---|
| Alcohol abuse/dependence | 13% to 26% | 32% (MS) | 6% |
| Depression | 18% to 40% |
58% (MS) 17% to 48% (R/F) | 6.6% |
| Suicidal ideation | 5% to 9% | 10% (MS) | 3.7% |
Among physicians, alcohol abuse/dependence has been significantly associated with the number of hours worked—a key cause of burnout—as well as with burnout itself [41,43,71,72,73]. Alcohol abuse/dependence is a substantial concern for physicians, as the rate reported in most studies has been much higher than that within the general population and is even higher among medical students [43,71,72,73,74]. In one study, burned out surgeons had a 25% increased risk of alcohol abuse or dependence [72]. However, in the 2015 Medscape survey, alcohol abuse was not prevalent, with approximately 50% of respondents reporting that they had less than one drink per day [47]. There was no difference in that study between physicians who were and were not burned out with regard to alcohol use [47]. In the 2019 Medscape survey, 23% of respondents reported drinking alcohol in order to cope with the effects of burnout [47].
As with alcohol abuse, the rates of depression and suicidal ideation are substantially higher in physicians than within the general population [30,36,49,75,76]. Few studies have been done to evaluate the relationship between burnout and depression or suicidal ideation. In one study of attending and resident emergency medicine physicians, burnout was significantly associated with a positive screen for depression [28]. In another study, persistent burnout during residency was associated with screening positively for depression as an intern [35]. Burnout has also been independently associated with suicidal ideation among surgeons and medical students [33,77]. However, the authors of most studies have gathered information on depression and burnout but have not analyzed the relationship. In most of these studies, rates of both depression and burnout have been high (Table 7) [34,40,43,49]. In another study, the rates of suicidal ideation and burnout were high among general internists (9% and 52%, respectively) [40].
Burnout and dissatisfaction with work-life balance have been reported to be the strongest predictors of intent to reduce clinical work hours or leave the current position [58]. In a 2019 study, it was found that burnout in the form of physician turnover and fewer available clinic hours resulted in costs of approximately $4.6 billion [122]. A systematic review provided evidence that burnout is associated with decreased productivity, defined as inability to work, increased number of sick days, and intent to leave practice or to change jobs [78]. Similarly, a review of physicians' administrative/payroll records showed that burnout scores correlated with reductions in professional effort (measured in full-time equivalent units) over the subsequent two years [79]. Specifically, the authors found that for each 1-point increase on the emotional exhaustion scale of the MBI, the likelihood of reducing work effort increased [79]. In one study, burned out physicians were significantly more likely than nonburned-out physicians to say that they intended to leave their practice within two years [29].
The authors of one study evaluated the number of years hospitalists intended to remain in practice in relation to risk of burnout; the percentage of hospitalists who intended to leave practice in less than four years ranged from 6.4% of those with no risk of burnout to 16.5% for those at risk for burnout to 44% for those who were burned out [80]. Another study was designed to evaluate burnout according to career stage; the physicians most likely to leave practice were those in middle-career, for whom rates of burnout were higher than for early- or late-career physicians. Approximately 12% of middle-career physicians said they planned to leave practice, compared with 5% of early- and late-career physicians [51]. The findings of all of these studies have implications for the supply of physicians, which is projected to fall short of the demand by 46,900 to 121,900 by the year 2032 [81].
Studies have also addressed the effect of physician burnout on medical errors, quality of care, and patient satisfaction [118]. One of the first of these studies involved internal medicine residents who were surveyed with the MBI and asked to respond to five statements regarding suboptimal care (e.g., "I did not fully discuss treatment options or answer a patient's questions" or "I made…errors that were not due to a lack of knowledge or inexperience") [32]. Approximately 53% of burned out residents self-reported suboptimal care compared with 21% of nonburned-out residents. In multivariate analyses, burnout was strongly associated with self-report of suboptimal care at least monthly. The authors also evaluated each domain of burnout and found that only a high score on the depersonalization domain was associated with suboptimal care. An association between high burnout scores and self-reports of suboptimal care and of medical errors was also found in later studies involving residents [41,82]. In one of these studies, self-reported medical errors and scores for best practices (following principles identified as best practices in anesthesiology) were significantly associated with high risk of burnout among anesthesiology residents [41]. The median best practice score was significantly lower for residents at high risk of burnout than for residents at low risk. In addition, significantly more residents at high risk for both burnout and depression reported multiple medical errors within the previous year compared with residents at low risk (33% vs. 0.7%) [41].
Burnout was also associated with self-reports of suboptimal care in a study of emergency medicine physicians and residents. The authors completed a burnout evaluation and asked six questions to assess suboptimal care; physicians who had high burnout scores were more likely to report all six acts of suboptimal care [28]. In another study, reporting a major medical error during the last three months was significantly associated with burnout among surgeons [83]. The depersonalization domain had the most effect; for each 1-point increase in the score in this domain, there was an 11% increase in the likelihood of reporting an error, and for each 1-point increase in the score on the emotional exhaustion scale, there was a 5% increase in likelihood. In multivariate analysis that controlled for other personal and professional factors, burnout was an independent predictor of reporting a major medical error. In contrast to these findings, studies of family physicians and general internists have shown no consistent relationships between burnout, medical errors, and quality of care [29,54].
With regard to patient satisfaction, a preliminary study involved a survey of 178 matched pairs of physicians and patients who had been hospitalized in the previous year. The authors found that a high score on the depersonalization domain was associated with lower rate of patient satisfaction and longer recovery after hospital discharge (after controlling for factors such as severity of illness) [84].
There are two primary approaches to preventing and/or coping with stress and burnout. Given that the most significant factors in burnout are related to the work environment, modifying the environment to eliminate these factors has the potential for the most success. However, it is often difficult to change organizational structure, which means individuals must make changes themselves. When implemented appropriately, prevention of burnout is easier and more cost-effective than resolving it once it has occurred; burnout that is addressed in later stages may take months or years to resolve fully [6,9]. Thus, the primary goal is to stop the burnout cycle early by preventing the accumulation of stress. Early recognition of stress is key to prevention [85]. However, several issues create challenges for physicians to prevent stress and burnout: misinterpretation of their own well-being, reluctance to seek help, and disinclination to care for themselves as a priority.
Although recognition of stress is important, physicians have been shown to inaccurately define their own well-being. Shanafelt et al. evaluated surgeons with the Mayo Clinic Physician Well-Being Index and then asked the surgeons to subjectively assess their well-being relative to other physicians [86]. Approximately 89% of the surgeons said that their well-being was at or above average, but 71% of the surgeons who scored in the bottom 30% on the Index relative to national physician norms had said their well-being was at or above average.
Many physicians do not seek help for stress or burnout because of the belief that these conditions are normal for the profession, an attitude that begins in medical school, with students being advised to push through stress [20,86]. This attitude leads physicians to believe that if they just work longer hours, the situation will resolve, but working longer hours only exacerbates stress and accelerates the burnout process. In addition, not dealing with stress appropriately may lead to factors associated with stress, such as alcohol abuse, depression, and suicide ideation. Despite the high rates of these conditions, studies have shown that 33% to 60% of medical students and physicians are reluctant to seek help [27,43,77]. The reasons for the reluctance are concerns about their medical license, discrimination in hospital privileges and professional advancement, perceived stigma, and an inability to take time off from work [27,43,45,87]. To help overcome these barriers, the Joint Commission issued guidelines mandating that medical staff "implement a process to identify and manage matters of individual health for licensed independent practitioners that is separate from actions taken for disciplinary purposes" [88].
The concept of self-care is emphasized in every book or article on preventing job stress and burnout across occupations. Self-care warrants particular emphasis for physicians, as they have been trained to put the care of others ahead of themselves and are not typically good at caring for themselves [89]. Self-care is essential for energizing, restoring, and maintaining the physical and emotional stamina to manage stress and helps increase job satisfaction [6,44,90].
The following strategies to prevent stress and burnout are recommended on the basis of studies of interventions as well as guidance from burnout experts and physicians who have successfully prevented stress and burnout. The strategies address changes in personal and professional lifestyle habits.
The most important first step in preventing stress and burnout is to enhance well-being. Self-care, improving work-life balance, and mindfulness training and other structured interventions are key elements for maintaining physical and emotional well-being (Table 8) [19,65,90,91,92,93,94]. Enhancing physicians' well-being is vital not only to address the consequences of stress and burnout but also to improve patient outcomes. The relationship between physician well-being and patient outcomes is understudied, but a systematic review (18 studies) showed that well-being was associated positively with patient satisfaction, patient adherence to treatment, and interpersonal aspects of patient care [95]. The authors of the review noted that most of the studies were observational and of average quality.
STRATEGIES FOR MANAGING STRESS AND AVOIDING BURNOUT
| Strategy Classification | Specific Strategies | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Personal lifestyle |
| ||||||||||
| Professional lifestyle |
| ||||||||||
| Organizational level |
|
Make Self-Care a Priority
Self-care involves several universal lifestyle measures, such as healthy eating habits, exercise, sleep, and regular health care. The results of studies and surveys have shown that physicians who maintain a healthy diet and follow the Centers for Disease Control and Prevention guidelines for exercise are less likely to be burned out [31,92,96]. Physicians who have successfully avoided burnout recommend self-care as a strategy, with physical well-being ranked as the most common strategy (60%) in a small study of hospice and palliative care physicians [93,94].
Attention to self-care should begin in medical training, and one program was developed to help second-year medical students focus better on personal behaviors, such as exercise, eating habits, sleep, and emotional health. The students were asked to target a specific area for change, set a goal, track their progress toward the goal, and assess their success [97]. Although approximately 50% of the students had not reached their goal by the end of the program, 80% said they were healthier because of the program and 82% said they would use the program again. Such programs during medical training can help foster self-care as a priority.
Improve Work-Life Balance
As noted, work-life balance and work-life conflicts are significantly associated with job satisfaction and burnout. One challenge in achieving an appropriate work-life balance is that physicians often search for a single solution to solve the problem. Drummond, who coaches physicians on how to avoid burnout, notes that burnout is more of a dilemma and so requires ongoing strategies to ensure finding and maintaining an appropriate balance [98].
Physicians who participate regularly in hobbies, personal interests, and meaningful volunteerism are at lower risk of burnout and are more likely to have higher quality of life [92,96]. Experts recommend scheduling time each week to pursue hobbies and participate in activities of interest [92,99,100]. Participating in hobbies was reported by 40% of physicians as a way they avoid burnout [94].
Other strategies include setting strict boundaries between work and home, making time for friends and family, taking regular vacations, and remaining clear about priorities [65,93,94,99]. Personal relationships and personal boundaries were reported by 37% (each) of physicians as a way to avoid burnout. As practical advice, Drummond suggests that physicians work with their families to develop a master "life calendar" that includes not only social events such as having coffee with a friend, reading, and exercise, but also all family members' schedules and special events [100]. Physicians should keep an electronic calendar or take a picture of the calendar with their cell phone, check the calendar when a potential work commitment arises, and learn to say no to colleagues' requests when necessary.
Engage in Mindfulness Training
Mindfulness is defined as purposeful and nonjudgmental attention to one's own experience, thoughts, and feelings [101]. Interventions to enhance mindfulness in primary care physicians have led to short-term and sustained improvements in well-being, reductions in indicators of stress and depression, and lower scores on the emotional exhaustion and depersonalization scales of the MBI [102,103]. A nine-month intervention that involved facilitated physician discussion groups that integrated elements of mindfulness with reflection, shared experience, and small-group learning significantly decreased scores on the depersonalization subscale that was sustained 12 months after the end of the program [104]. Scores on the emotional exhaustion subscale and overall burnout scores also decreased substantially. The intervention improved physicians' sense of meaning in their work but did not lead to significant differences in stress, symptoms of depression, or job satisfaction [104]. Mindfulness has also been associated with more patient-centered communication and an increase in the number of satisfied patients [101].
Explore Other Interventions
Cognitive-behavioral training, physical relaxation (e.g., massage), and mental relaxation (e.g., mediation) may have limited benefit, according to a meta-analysis of interventions to reduce work-related stress in healthcare workers. The study demonstrated low-quality evidence that cognitive-behavioral training, with or without relaxation, reduced stress compared with no intervention, but only after the more than one month of follow-up [105]. Similarly, physical relaxation was most effective one to six months after the intervention. Little evidence supported mental relaxation as a way to reduce work-related stress after up to six months [105].
As discussed, use of EHRs is a leading source of physicians' stress and dissatisfaction, and approximately 61% of physicians have reported that other staff could perform functions in EHRs [37]. Thus, making documentation a team effort can help alleviate physicians' electronic burden. In addition, experts recommend that physicians ask colleagues for help in using EHRs more efficiently and that they create templates as a way to semiautomate documentation [98,106].
Given that a chaotic work environment is associated with high rates of stress, job dissatisfaction, and burnout, eliminating chaos can help prevent stress and burnout [65]. Redesigning work flow can also help; this strategy was associated with significant reductions in the burnout rate in a study of primary care clinicians working at 34 clinics [107].
Physicians can work more efficiently by standardizing workflows and processes whenever possible, minimizing interruptions by batching nonurgent tasks, and creating patient resources or delegating patient education [98]. Taking mini-breaks during the day gives physicians time to recharge and refocus [108].
Physicians can take steps in their practice to promote a healthy work environment, and physicians in hospitals or managed care settings should work with leaders to ensure that all physicians and staff have a healthy work environment [19]. Flexible scheduling is an important element of a healthy work environment, as it gives physicians better control over their time and helps them achieve greater satisfaction with work-life balance [52,108].
Participate in Support Groups
Support from colleagues can help to increase job satisfaction and reduce the likelihood of burnout [44,80,109]. In one study, professional relationships were the second most common strategy for preventing burnout, reported by 57% of physicians [94]. Physicians are often hesitant to seek help, but such support groups are not designed to be solely for physicians with mental health or substance abuse issues. Instead, support groups offer an opportunity for healthy but stressed physicians to discuss professional and personal problems [90]. Two randomized trials have demonstrated that programs offering physicians an opportunity to meet with colleagues in a structured format substantially reduced the rate of burnout and enhanced physician engagement [104,110].
Support groups can also focus on a theme. For example, residents rotating through a medical intensive care unit developed "grief rounds" as a way to discuss their feelings and other issues related to the deaths of patients they cared for [111]. When asked to assess the program, 77% of respondents agreed or strongly agreed that the rounds enhanced their intensive care unit experience. Further study is planned to determine if the grief rounds are associated with a decrease in burnout.
Pursue Professional Passions
Administrative burden and heavy patient loads often reduce the amount of time physicians have to pursue their professional passions, but time to participate in specific clinical or research interests is essential to having meaningful work, which in turn is paramount to physicians' satisfaction [20,92,112]. In the 2015 Medscape survey, lack of professional fulfillment was a leading cause of burnout [31]. Surgeons who focus on finding greater meaning in work have been less likely to become burned out, and other physicians have noted that maintaining passion for one's work is helpful in avoiding burnout [94,96].
Encourage Organizational Change
Physicians should work with leaders to effect organizational change that addresses issues associated with job dissatisfaction and burnout, such as excessive hours or workload, inefficiency, electronic burden, lack of physician autonomy, and inadequate resources for high-quality care and patient safety [20,112,113,114]. Physicians can become advocates for making these changes as well as other strategies, such as promoting part-time careers for physicians, providing protected time for physicians to pursue meaningful professional activities, offering programs that enhance physicians' resiliency (such as mindfulness programs) and provide opportunities for physicians to interact with their colleagues, making physician satisfaction and well-being quality indicators, and emphasizing the importance of self-care [20,114,115]. It is vital that physicians are true partners with leaders in collaborating for such changes [112].
Physicians can become champions of a healthy work environment by developing or participating in a wellness committee. This committee should be composed of physicians, other healthcare professionals, and staff and should collaborate with the organization's leaders [108]. Some potential initiatives are opportunities for physicians to openly and honestly discuss medical errors, how to achieve well-being, and how to avoid stress [65]. A wellness committee can also work to ensure that tools are available to assess physician well-being and burnout and that the results generate resources to address physicians' needs.
The substantial effect of stress, dissatisfaction, and burnout has led some professional organizations to publish position papers or calls for action. For example, the American Academy of Family Physicians published a position paper to note its commitment to helping find personal and system-wide solutions to physician burnout [116]. The Critical Care Societies Collaborative issued a call for action to enhance awareness of burnout in the critical care specialty and to encourage members of the specialty to work to create a healthy work environment [19]. The American Academy of Pediatrics issued a call to prevent burnout by promoting physician health and wellness, and the American Medical Association developed the program STEPS Forward as a resource to help physicians address practice-related issues that have been associated with burnout [85,117]. In a collaborative report by the Massachusetts Medical Society, the Massachusetts Health and Hospital Association, the Harvard T.H. Chan School of Public Health, and the Harvard Global Health Institute, physician burnout is declared to be a public health crisis, seriously impacting "the health and well-being of the American public" [120]. The call to action lays out a plan of intervention to help reduce physician burnout.
Burnout is a syndrome of emotional exhaustion, depersonalization, and reduced personal accomplishment. Levels of burnout are high among physicians, ranging from 27% to 60%, with even higher rates among physicians in training. At the root of burnout is job dissatisfaction. If left unaddressed, this dissatisfaction can lead to prolonged stress and subsequent burnout. Several causes of burnout among physicians have been identified, including work overload; long hours; inadequate work-life balance; excessive time for administrative tasks, especially electronic documentation; loss of autonomy; and evolving health policy. These sources of dissatisfaction can be correlated with mismatches identified by Maslach, the foremost authority on burnout.
High degrees of job dissatisfaction and stress precede burnout, making it incumbent on physicians to recognize stress early to help prevent burnout before it occurs. Preventing burnout is vital not only for the well-being and professional preservation of physicians but also for ensuring optimal patient outcomes. Several personal and professional lifestyle strategies can help physicians cope with stress, achieve better work-life balance, and become more engaged in their work. Practices and institutions should focus on creating a healthy work environment in which physicians feel supported by their peers, have control over their schedules as well as decision-making regarding their patients, and are offered resources to help them develop resiliency and enhance their well-being.
1. American Institute of Stress. What the Latest Reports Say About Stress in America. Available at https://www.stress.org/news/what-the-latest-reports-say-about-stress-in-america/. Last accessed September 3, 2025.
2. American Psychological Association. 2023 Work in America Survey. Available at https://www.apa.org/pubs/reports/work-in-america/2023-workplace-health-well-being. Last accessed September 3, 2025.
3. Felton J. Burnout as a clinical entity: its importance in health care workers. Occup Med (Lond). 1998;48(4):237-250.
5. Edelwich J, Brodsky A. Burn-out: Stages of Disillusionment in the Helping Professions. New York, NY: Springer; 1980.
7. Maslach C, Jackson SE, Leiter MP. Maslach Burnout Inventory Manual. 2nd ed. Palo Alto, CA: Consulting Psychologists Press; 1986.
8. Maslach C, Jackson SE, Leiter MP. Maslach Burnout Inventory Manual. 4th ed. Palo Alto, CA: Consulting Psychologists Press; 2018.
9. Maslach C, Leiter MP. The Truth about Burnout: How Organizations Cause Personal Stress and What to Do About It. San Francisco, CA: Jossey-Bass; 1997.
10. Purvanova R, Muros JP. Gender differences in burnout: a meta-analysis. J Vocat Behav. 2010;77(2):168-185.
11. Shanafelt T, Boone S, Tan L, et al. Burnout and satisfaction with work-life balance among U.S. physicians relative to the general U.S. population. Arch Intern Med. 2012;172(18):1377-1385.
12. Keidel GC. Burnout and compassion fatigue among hospice caregivers. Am J Hosp Palliat Care. 2002;19(3):200-205.
13. Denollet J. DS14: standard assessment of negative affectivity, social inhibition, and type D personality. Psychosom Med. 2005;67(1):89-97.
14. Ogńska-Bulik N. Occupational stress and its consequences in healthcare professionals: the role of type D personality. Int J Occup Med Environ Health. 2006;19(2):113-122.
15. Leone SS, Huibers MJH, Knottnerus JA, Kant IJ. Similarities, overlap and differences between burnout and prolonged fatigue in the working population. QJM. 2007;100(10):617-627.
16. Leone S, Huibers MJ, Knottnerus JA, Kant I. The prognosis of burnout and prolonged fatigue in the working population: a comparison. J Occup Environ Med. 2008;50(10):1195-1202.
17. Brenninkmeijer V VN, Buunk BP. Burnout and depression are not identical twins: is decline of superiority a distinguishing feature? Personality Individ Diff. 2001;30(5):873-880.
18. Ahola K, Hakanen J, Perhoniemi R, Mutanen P. Relationship between burnout and depressive symptoms: a study using the person-centred approach. Burnout Res. 2014;1(1):29-37.
19. Moss M, Good VS, Gozal D, Kleinpell R, Sessler CN. An official critical care societies collaborative statement: burnout syndrome in critical care health care professionals: a call for action. Am J Crit Care. 2016;25(4):368-376.
20. Hlubocky FJ, Back AL, Shanafelt TD. Addressing burnout in oncology: why cancer care clinicians are at risk, what individuals can do, and how organizations can respond. Am Soc Clin Oncol Educ Book. 2016;35:271-279.
21. Rohland BM, Kruse GR, Rohrer JE. Validation of a single-item measure of burnout against the Maslach Burnout Inventory among physicians. Stress Health. 2004;20(2):75-79.
22. West CP, Dyrbye LN, Satele DV, Sloan JA, Shanafelt TD. Concurrent validity of single-item measures of emotional exhaustion and depersonalization in burnout assessment. J Gen Intern Med. 2012;27(11):1445-1452.
23. Dolan ED, Mohr D, Lempa M, et al. Using a single item to measure burnout in primary care staff: a psychometric evaluation. J Gen Intern Med. 2015;30(5):582-587.
24. Dyrbye LN, Satele D, Sloan J, Shanafelt TD. Utility of a brief screening tool to identify physicians in distress. J Gen Intern Med. 2013;28(3):421-427.
26. Linzer M, Gerrity M, Douglas JA, McMurray JE, Williams ES, Konrad TR; the Society of General Internal Medicine (SGIM) Career Satisfaction Study Group. Physician stress: results from the Physician Worklife Study. Stress Health. 2002;18(1):37-42.
27. Dyrbye LN, Eacker A, Durning SJ, et al. The impact of stigma and personal experiences on the help-seeking behaviors of medical students with burnout. Acad Med. 2015;90(7):961-969.
28. Lu DW, Dresden S, McCloskey C, Branzetti J, Gisondi MA. Impact of burnout on self-reported patient care among emergency physicians. West J Emerg Med. 2015;16(7):996-1001.
29. Rabatin J, Williams E, Baier Manwell L, Schwartz MD, Brown RL, Linzer M. Predictors and outcomes of burnout in primary care physicians. J Prim Care Community Health. 2016;7(1):41-43.
30. Shanafelt T, Hasan O, Dyrbye LN, et al. Changes in burnout and satisfaction with work-life balance in physicians and the general U.S. working population between 2011 and 2014. Mayo Clin Proc. 2015;90(12):1600-1613.
31. Peckham C. Physician Burnout: It Just Keeps Getting Worse. Available at https://www.medscape.com/viewarticle/838437. Last accessed September 24, 2025.
32. Shanafelt T, Bradley KA, Wipf JE, Back AL. Burnout and self-reported patient care in an internal medicine residency program. Ann Intern Med. 2002;136(5):358-367.
33. Dyrbye LN, Thomas MR, Massie FS, et al. Burnout and suicidal ideation among U.S. medical students. Ann Intern Med. 2008;149(5):334-341.
34. Shanafelt T, Balch CM, Bechamps GJ, et al. Burnout and career satisfaction among American surgeons. Ann Surg. 2009;250(3):463-471.
35. Campbell J, Prochazka AV, Yamashita T, Gopal R. Predictors of persistent burnout in internal medicine residents: a prospective cohort study. Acad Med. 2010;85(10):1630-1634.
36. Balch C, Shanafelt TD, Sloan J, Satele DV, Kuerer HM. Burnout and career satisfaction among surgical oncologists compared with other surgical specialties. Ann Surg Oncol. 2011;18(1):16-25.
37. Friedberg M, Chen PG, Van Busum KR, et al. Factors Affecting Physician Professional Satisfaction and Their Implications for Patient Care, Health Systems, and Health Policy. Available at https://www.rand.org/pubs/research_reports/RR439.html. Last accessed September 24, 2025.
38. West CP, Halvorsen AJ, Swenson SL, McDonald FS. Burnout and distress among internal medicine program directors: results of a national survey. J Gen Intern Med. 2013;28(8):1056-1063.
39. Arora M, Diwan AD, Harris IA. Burnout in orthopaedic surgeons: a review. ANZ J Surg. 2013;83(7-8):512-515.
40. Roberts DL, Shanafelt TD, Dyrbye LN, West CP. A national comparison of burnout and work-life balance among internal medicine hospitalists and outpatient general internists. J Hosp Med. 2014;9(3):176-181.
41. de Oliveira GS Jr, Chang R, Fitzgerald PC, et al. The prevalence of burnout and depression and their association with adherence to safety and practice standards: a survey of United States anesthesiology trainees. Anesth Analg. 2013;117(1):182-193.
42. Shanafelt T, Gradishar WJ, Kosty M, et al. Burnout and career satisfaction among US oncologists. J Clin Oncol. 2014;32(7):678-686.
43. Rath K, Huffman LB, Phillips GS, Carpenter KM, Fowler JM. Burnout and associated factors among members of the Society of Gynecologic Oncology. Am J Obstet Gynecol. 2015;213(6):824.e821-829.
44. Starmer AJ, Frintner MP, Freed GL. Work-life balance, burnout, and satisfaction of early career pediatricians. Pediatrics. 2016;137(4).
45. Holmes EG, Connolly A, Putnam KT, et al. Taking care of our own: a multispecialty study of resident and program director perspectives on contributors to burnout and potential interventions. Acad Psychiatry. 2017;41(2):159-166.
46. Elmore LC, Jeffe DB, Jin L, Awad MM, Turnbull IR. National survey of burnout among U.S. general surgery residents. J Am Coll Surg. 2016;223(3):440-451.
47. Kane L. Medscape National Physician Burnout, Depression, and Suicide Report 2019. Available at https://www.medscape.com/slideshow/2019-lifestyle-burnout-depression-6011056. Last accessed September 24, 2025.
48. Dyrbye LN, Shanafelt TD, Balch CM, Satele D, Sloan J, Freischlag J. Relationship between work-home conflicts and burnout among American surgeons: a comparison by sex. Arch Surg. 2011;146(2):211-217.
49. Dyrbye LN, West CP, Satele D, et al. Burnout among U.S. medical students, residents, and early career physicians relative to the general U.S. population. Acad Med. 2014;89(3):443-451.
50. Pulcrano M, Evans SR, Sosin M. Quality of life and burnout rates across surgical specialties: a systematic review. JAMA Surg. 2016;151(10):970-978.
51. Dyrbye LN, Varkey P, Boone SL, Satele DV, Sloan JA, Shanafelt TD. Physician satisfaction and burnout at different career stages. Mayo Clin Proc. 2013;88(12):1358-1367.
52. Shanafelt T, Sloan JA, Habermann TM. The well-being of physicians. Am J Med Qual. 2003;114(6):513-519.
53. Physicians Foundation. 2018 Survey of America's Physicians: Practice Patterns and Perspectives. Available at https://physiciansfoundation.org/wp-content/uploads/2018/09/physicians-survey-results-final-2018.pdf. Last accessed September 24, 2025.
54. Linzer M, Manwell LB, Williams ES, et al. Working conditions in primary care: physician reactions and care quality. Ann Intern Med. 2009;151(1):28-36.
55. Leigh JP, Tancredi D, Jerant A, Kravitz RL. Annual work hours across physician specialties. Arch Intern Med. 2011;171(13):1211-1213.
56. Linzer M, Poplau S, Babbott S, et al. Worklife and wellness in academic general internal medicine: results from a national survey. J Gen Intern Med. 2016;31(9):1004-1010.
57. Woolhandler S, Himmelstein DU. Administrative work consumes one-sixth of U.S. physicians' working hours and lowers their career satisfaction. Int J Health Serv. 2014;44(4):635-642.
58. Shanafelt TD, Raymond M, Kosty M, et al. Satisfaction with work-life balance and the career and retirement plans of U.S. oncologists.J Clin Oncol. 2014;32(11):1127-1135.
59. Jamoom E, Patel V, King J Furukawa MF. Physician Experience with Electronic Health Record Systems that Meet Meaningful Use Criteria: NAMCS Physician Workflow Survey, 2011. Hyattsville, MD: National Center for Health Statistics; 2013.
60. Hill RG Jr, Sears LM, Melanson SW. 4000 Clicks: a productivity analysis of electronic medical records in a community hospital ED. Am J Emerg Med. 2013;31(11):1591-1594.
61. Shanafelt TD, Dyrbye LN, Sinsky C, et al. Relationship between clerical burden and characteristics of the elctronic environment with physician burnout and professional satisfaction. Mayo Clin Proc. 2016;91(7):836-848.
62. Babbott S, Manwell LB, Brown R, et al. Electronic medical records and physician stress in primary care: results from the MEMO study. J Am Med Inform Assoc. 2014;21(e1):e100-e106.
63. Ariely D, Lanier WL. Disturbing trends in physician burnout and satisfaction with work-life balance: dealing with malady among the nation's healers. Mayo Clin Proc. 2015;90(12):1593-1596.
64. Stoddard JJ, Hargraves JL, Reed M, Vratil A. Managed care, professional autonomy, and income: effects on physician career satisfaction. J Gen Intern Med. 2001;16(10):675-684.
65. Vassar L. How to Beat Burnout: 7 Signs Physicians Should Know. Available at https://www.ama-assn.org/practice-management/physician-health/how-beat-burnout-7-signs-physicians-should-know. Last accessed September 24, 2025.
66. Street D, Cossman J. Health Workforce Brief: Autonomy, Satisfaction and Physician Burnout. Available at https://www.researchgate.net/publication/254871039_Autonomy_Satisfaction_and_Physician_Burnout. Last accessed September 24, 2025.
67. Schrijver I, Brady KJ, Trockel M. An exploration of key issues and potential solutions that impact physician wellbeing and professional fulfillment at an academic center. Peer J. 2016;4:e1783.
68. Kimo Takayesu J, Ramoska EA, Clark TR, et al. Factors associated with burnout during emergency medicine residency. Acad Emerg Med. 2014;21(9):1031-1035.
69. Karsh BT, Beasley JW, Brown RL. Employed family physician satisfaction and commitment to their practice, work group, and health care organization. Health Serv Res. 2010;45(2):457-475.
70. Balch CM, Oreskovich MR, Dyrbye LN, et al. Personal consequences of malpractice lawsuits on American surgeons. J Am Coll Surg. 2011;213(5):657-667.
71. Oreskovich MR, Shanafelt TD, Dyrbye LN, et al. The prevalence of substance use disorders in American physicians. Am J Addict. 2015;24(1):30-38.
72. Oreskovich M, Kaups KL, Balch CM, et al. Prevalence of alcohol use disorders among American surgeons. Arch Surg. 2012;147(2):168-174.
73. Jackson ER, Shanafelt TD, Hasan O, Satele DV, Dyrbye LN. Burnout and alcohol abuse/dependence among U.S. medical students. Acad Med. 2016;91(9):1251-1256.
74. National Center for Health Statistics. Health, United States, 2017. Available at https://www.cdc.gov/nchs/data/hus/hus17.pdf. Last accessed September 25, 2025.
75. National Institute of Mental Health. Major Depression. Available at https://www.nimh.nih.gov/health/statistics/major-depression.shtml. Last accessed September 25, 2025.
76. Crosby A, Han B, Ortega LAG, Parks SE, Gfroerer J. Suicidal thoughts and behaviors among adults aged ≥18 Years—United States, 2008–2009. MMWR Surveill Summ. 2011;60(13):1-22.
77. Shanafelt TD, Balch CM, Dyrbye L, et al. Special report: suicidal ideation among American surgeons. Arch Surg. 2011;146(1): 54-62.
78. Dewa CS, Loong D, Bonato S, Thanh NX, Jacobs P. How does burnout affect physician productivity? A systematic literature review. BMC Health Serv Res. 2014;14:325.
79. Shanafelt TD, Mungo M, Schmitgen J, et al. Longitudinal study evaluating the association between physician burnout and changes in professional work effort. Mayo Clin Proc. 2016;91(4):422-431.
80. Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. J Health Soc Behav. 2002;43(1):72-91.
81. IHS, Inc. 2019 Update: The Complexities of Physician Supply and Demand: Projections from 2017 to 2032. Washington, DC: Association of American Medical Colleges; 2019.
82. Block L, Wu AW, Feldman L, Yeh HC, Desai SV. Residency schedule, burnout and patient care among first-year residents. Postgrad Med J. 2013;89(1005):495-500.
83. Shanafelt TD, Balch CM, Bechamps G, et al. Burnout and medical errors among American surgeons. Ann Surg. 2010;251(6):995-1000.
84. Halbesleben JR, Rathert C. Linking physician burnout and patient outcomes: exploring the dyadic relationship between physicians and patients. Health Care Manage Rev. 2008;33(1):29-39.
85. McClafferty H, Brown OW, Section on Integrative Medicine, Committee on Practice and Ambulatory Medicine. Physician health and wellness. Pediatrics. 2014;134(4):830-835.
86. Shanafelt T, Kaups KL, Nelson H, et al. An interactive individualized intervention to promote behavioral change to increase personal well-being in U.S. surgeons. Ann Surg. 2014;259(1):82-88.
87. Center C, Davis M, Detre T, et al. Confronting depression and suicide in physicians: a consensus statement. JAMA. 2003;289(23): 3161-3166.
88. The Joint Commission. Comprehensive Accreditation Manual for Hospitals: The Official Handbook, 2011. Oakbrook Terrace, IL: The Joint Commission; 2011.
89. Wallace JE, Lemaire JB, Ghali WA. Physician wellness: a missing quality indicator. Lancet. 2009;374(9702):1714-1721.
90. Zeckhausen W. Eight ideas for managing stress and extinguishing burnout. Fam Pract Manag. 2002;9(4):35-38.
91. Nedrow A, Steckler NA, Hardman J. Physician resilience and burnout: can you make the switch? Fam Pract Manag. 2013;20(1): 25-30.
92. Vassar L. Burnout Busters: How to Boost Satisfaction in Personal Life, Practice. Available at https://www.ama-assn.org/practice-management/physician-health/burnout-busters-how-boost-satisfaction-personal-life-practice. Last accessed September 25, 2025.
93. Meldrum H. Exemplary physicians' strategies for avoiding burnout. Health Care Manag (Frederick). 2010;29(4):324-331.
94. Swetz KM, Harrington SE, Matsuyama RK, Shanfelt TD, Lyckholm LJ. Strategies for avoiding burnout in hospice and palliative medicine: peer advice for physicians on achieving longevity and fulfillment. J Palliat Med. 2009;12(9):773-777.
95. Scheepers RA, Boerebach BC, Arah OA, Heineman MJ, Lombarts KM. A systematic review of the impact of physicians' occupational well-being on the quality of patient care. Int J Behav Med. 2015;22(6):683-698.
96. Shanafelt TD, Oreskovich MR, Dyrbye LN, et al. Avoiding burnout: the personal health habits and wellness practices of U.S. surgeons. Ann Surg. 2012;255(4):625-633.
97. Kushner R, Kessler S, McGaghie WC. Using behavior change plans to improve medical student self-care. Acad Med. 2011;86(7):901-906.
98. Drummond D. Eight ways to lower practice stress and get home sooner. Fam Pract Manag. 2015;22(6):13-18.
99. Galinsky E, Families and Work Institute. Dual-Centric: A New Concept of Work-Life. Available at http://www.stemcareer.com/richfeller/pages/studenthelp/Documents/Dual Work Centric-A New Concept of Work-Life.pdf. Last accessed September 25, 2025.
100. Drummond D. Four tools for reducing burnout by finding work-life balance. Fam Pract Manag. 2016;23(1):28-33.
101. Beach MC, Roter D, Korthuis PT, et al. A multicenter study of physician mindfulness and health care quality. Ann Fam Med. 2013;11(5):421-428.
102. Krasner MS, Epstein RM, Beckman H, et al. Association of an educational program in mindful communication with burnout, empathy, and attitudes among primary care physicians. JAMA. 2009;302(12):1284-1293.
103. Fortney L, Luchterhand C, Zakletskaia L, Zgierska A, Rakel D. Abbreviated mindfulness intervention for job satisfaction, quality of life, and compassion in primary care clinicians: a pilot study. Ann Fam Med. 2013;11(5):412-420.
104. West CP, Dyrbye LN, Rabatin JT, et al. Intervention to promote physician well-being, job satisfaction, and professionalism: a randomized clinical trial. JAMA Intern Med. 2014;174(4):527-533.
105. Ruotsalainen J, Verbeek JH, Marine A, Serra C. Preventing occupational stress in healthcare workers. Cochrane Database Syst Rev. 2015;4:CD002892.
106. Bodenheimer T, Sinsky C. From triple to quadruple aim: care of the patient requires care of the provider. Ann Fam Med. 2014;12(6):573-576.
107. Linzer M, Poplau S, Grossman E, et al. A cluster randomized trial of interventions to improve work conditions and clinician burnout in primary care: results from the Healthy Work Place (HWP) study. J Gen Intern Med. 2015;30(8):1105-1111.
108. Linzer M, Guzman-Corrales L, Poplau S. AMA STEPS Forward Module: Preventing Physician Burnout. Available at https://edhub.ama-assn.org/steps-forward/module/2702509. Last accessed September 25, 2025.
109. Harolds JA, Parikh JR, Bluth EI, Dutton SC, Recht MP. Burnout of radiologists: frequency, risk factors, and remedies: a report of the ACR Commission on Human Resources. J Am Coll Radiol. 2016;13(4):411-416.
110. West CP, Dyrbye LN, Satele D, Shanafelt TD. A randomized controlled trial evaluating the effect of COMPASS (Colleagues Meeting to Promote and Sustain Satisfaction) small group sessions on physician well-being, meaning, and job satisfaction. J Gen Intern Med. 2015;30:S89.
111. Wilde L, Worster B, Oxman D. Monthly "grief rounds" to improve residents' experience and decrease burnout in a medical intensive care unit rotation. Am J Med Qual. 2016;31(4):379.
112. Swensen S, Kabcenell A, Shanafelt T. Physician-organization collaboration reduces physician burnout and promotes engagement: the Mayo Clinic experience. J Healthc Manag. 2016;61(2):105-127.
113. Shanafelt T, Dyrbye L. Oncologist burnout: causes, consequences, and responses. J Clin Oncol. 2012;30(11):1235-1241.
114. Linzer M, Levine R, Meltzer D, Poplau S, Warde C, West CP. 10 Bold steps to prevent burnout in general internal medicine. J Gen Intern Med. 2013;29(1):18-20.
115. Shapiro J, Galowitz P. Peer support for clinicans: a programmatic approach. Acad Med. 2016;91(9):1200-1204.
116. American Academy of Family Physicians. Physician Burnout (Position Paper). Available at https://www.aafp.org/about/policies/all/family-physician-burnout.html. Last accessed September 25, 2025.
117. American Medical Association. AMA Launches STEPS Forward to Address Physician Burnout. Available at https://www.ama-assn.org/press-center/press-releases/ama-launches-steps-forward-address-physician-burnout. Last accessed September 25, 2025.
118. Tawfik DS, Profit J, Morgenthaler TI, et al. Physician burnout, well-being, and work unit safety grades in relationship to reported medical errors. Mayo Clin Proc. 2018;93(11):1571-1580.
119. World Health Organization. ICD-11 for Mortality and Morbidity Statistics: QD85 Burn-out. Available at https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/129180281. Last accessed September 3, 2025.
120. Jha, AK, Iliff, AR, Chaoui, AA, Defossez, S, Bombaugh, MC, Miller, YR. A Crisis in Healthcare: A Call to Action on Physician Burnout. Available at https://cdn1.sph.harvard.edu/wp-content/uploads/sites/21/2019/01/PhysicianBurnoutReport2018FINAL.pdf. Last accessed September 3, 2025.
122. Han S, Shanafelt TD, Sinsky CA, Awad KM, Dyrbye LN, Fiscus LC, et al. Estimating the attributable cost of physician burnout in the United States. Ann Intern Med. 2019;170(11):784-790.
123. Physicians Foundation. 2021 Survey of America's Physicians COVID-19 Impact Edition: A Year Later. Available at https://physiciansfoundation.org/wp-content/uploads/2021/08/2021-Survey-Of-Americas-Physicians-Covid-19-Impact-Edition-A-Year-Later.pdf. Last accessed September 25, 2025.
124. Shanafelt TD, West CP, Dyrbye LN, et al. Changes in burnout and satisfaction with work-life integration in physicians over the first 2 years of the COVID-19 pandemic. Mayo Clin Proc. 2022; [Epub ahead of print].
125. Shanafelt TD, West CP, Sinsky C, et al. Changes in burnout and satisfaction with work-life integration in physicians and the general US working population between 2011 and 2020. Mayo Clin Proc. 2022;97(3):491-506.
126. Physicians Foundation. 2023 Survey of America's Current and Future Physicians. Available at https://physiciansfoundation.org/wp-content/uploads/PF23_Brochure-Report_Americas-Physicians_V2b-1-2.pdf. Last accessed September 5, 2025.
127. Physicians Foundation. Surveys. Available at https://physiciansfoundation.org/surveys. Last accessed September 5, 2025.
128. Medscape. Medscape National Physician Burnout and Depression Report 2018. Available at https://www.medscape.com/slideshow/2018-lifestyle-burnout-depression-6009235#6. Last accessed 9/21/2025.
129. Medscape. Medscape Physician Burnout & Depression Report 2024: "We Have Much Work to Do". Available at https://www.medscape.com/slideshow/2024-lifestyle-burnout-6016865#1. Last accessed September 23, 2015.
Mention of commercial products does not indicate endorsement.