Although obesity has been shown to be a risk factor for numerous diseases such as diabetes, coronary artery disease, and sleep apnea, most overweight and obese people do not consider themselves at higher risk for medical problems or premature death. News stories on various diets have caused confusion among many patients and health providers, leading to frustration and subsequent inaction. This course will help educate physicians and other healthcare professionals about the epidemiology and treatment of overweight and obese patients. Using current national guidelines, the clinical management of patients will be discussed. Clinical presentation, diagnosis, behavioral, and pharmacologic management will be reviewed. Surgical options for morbidly obese patients will also be examined. Steps to address and treat recidivism will be explored. Finally, current reimbursement issues will be discussed.
This course is designed for all physicians, nurses, and social work/counseling groups involved in the care of patients who are overweight or obese.
Obesity is epidemic in the United States. As statistics indicate that the problem is growing, the purpose of this course is to educate healthcare professionals about the epidemiology and treatment of overweight and obese patients. Clinical management, presentation, diagnosis, and behavioral and medical management will be reviewed to assist healthcare professionals in encouraging their patients to lose weight and prevent obesity-related comorbidities.
Upon completion of this course, you should be able to:
- Discuss the clinical background of obesity, noting the various definitions.
- Discuss the epidemiology of overweight and obese individuals in the United States, based on age, race, and socioeconomic status.
- Describe the pathophysiology of obesity, including genetic and environmental factors.
- Identify the risk factors for and comorbidities of obesity.
- Explain the various treatment modalities for overweight/obese patients.
- Describe dietary and physical activity recommendations.
- Discuss available pharmacologic agents, including indications and adverse reactions, used to treat obese/overweight patients.
- Discuss surgical options, including restriction and bypass operations.
- Outline considerations necessary when caring for patients for whom English is a second language.
John J. Whyte, MD, MPH, is currently the Chief Medical Officer at WebMD. In this role, he leads efforts to develop and expand strategic partnerships that create meaningful change around important and timely public health issues. Previously, Dr. Whyte was the Director of Professional Affairs and Stakeholder Engagement at the FDA’s Center for Drug Evaluation and Research and the Chief Medical Expert and Vice President, Health and Medical Education at Discovery Channel, part of the media conglomerate Discovery Communications.
Prior to this, Dr. Whyte was in the Immediate Office of the Director at the Agency for Healthcare Research Quality. He served as Medical Advisor/Director of the Council on Private Sector Initiatives to Improve the Safety, Security, and Quality of Healthcare. Prior to this assignment, Dr. Whyte was the Acting Director, Division of Medical Items and Devices in the Coverage and Analysis Group in the Centers for Medicare & Medicaid Services (CMS). CMS is the federal agency responsible for administering the Medicare and Medicaid programs. In his role at CMS, Dr.Whyte made recommendations as to whether or not the Medicare program should pay for certain procedures, equipment, or services. His division was responsible for durable medical equipment, orthotics/prosthetics, drugs/biologics/therapeutics, medical items, laboratory tests, and non-implantable devices. As Division Director as well as Medical Officer/Senior Advisor, Dr. Whyte was responsible for more national coverage decisions than any other CMS staff.
Dr. Whyte is a board-certified internist. He completed an internal medicine residency at Duke University Medical Center as well as earned a Master’s of Public Health (MPH) in Health Policy and Management at Harvard University School of Public Health. Prior to arriving in Washington, Dr. Whyte was a health services research fellow at Stanford and attending physician in the Department of Medicine. He has written extensively in the medical and lay press on health policy issues.
Contributing faculty, John J. Whyte, MD, MPH, has disclosed no relevant financial relationship with any product manufacturer or service provider mentioned.
John M. Leonard, MD
John V. Jurica, MD, MPH
Mary Franks, MSN, APRN, FNP-C
Alice Yick Flanagan, PhD, MSW
Margaret Donohue, PhD
Randall L. Allen, PharmD
The division planners have disclosed no relevant financial relationship with any product manufacturer or service provider mentioned.
Sarah Campbell
The Director of Development and Academic Affairs has disclosed no relevant financial relationship with any product manufacturer or service provider mentioned.
The purpose of NetCE is to provide challenging curricula to assist healthcare professionals to raise their levels of expertise while fulfilling their continuing education requirements, thereby improving the quality of healthcare.
Our contributing faculty members have taken care to ensure that the information and recommendations are accurate and compatible with the standards generally accepted at the time of publication. The publisher disclaims any liability, loss or damage incurred as a consequence, directly or indirectly, of the use and application of any of the contents. Participants are cautioned about the potential risk of using limited knowledge when integrating new techniques into practice.
It is the policy of NetCE not to accept commercial support. Furthermore, commercial interests are prohibited from distributing or providing access to this activity to learners.
Supported browsers for Windows include Microsoft Internet Explorer 9.0 and up, Mozilla Firefox 3.0 and up, Opera 9.0 and up, and Google Chrome. Supported browsers for Macintosh include Safari, Mozilla Firefox 3.0 and up, Opera 9.0 and up, and Google Chrome. Other operating systems and browsers that include complete implementations of ECMAScript edition 3 and CSS 2.0 may work, but are not supported. Supported browsers must utilize the TLS encryption protocol v1.1 or v1.2 in order to connect to pages that require a secured HTTPS connection. TLS v1.0 is not supported.
The role of implicit biases on healthcare outcomes has become a concern, as there is some evidence that implicit biases contribute to health disparities, professionals' attitudes toward and interactions with patients, quality of care, diagnoses, and treatment decisions. This may produce differences in help-seeking, diagnoses, and ultimately treatments and interventions. Implicit biases may also unwittingly produce professional behaviors, attitudes, and interactions that reduce patients' trust and comfort with their provider, leading to earlier termination of visits and/or reduced adherence and follow-up. Disadvantaged groups are marginalized in the healthcare system and vulnerable on multiple levels; health professionals' implicit biases can further exacerbate these existing disadvantages.
Interventions or strategies designed to reduce implicit bias may be categorized as change-based or control-based. Change-based interventions focus on reducing or changing cognitive associations underlying implicit biases. These interventions might include challenging stereotypes. Conversely, control-based interventions involve reducing the effects of the implicit bias on the individual's behaviors. These strategies include increasing awareness of biased thoughts and responses. The two types of interventions are not mutually exclusive and may be used synergistically.
#91574: Diagnosing and Treating Overweight and Obese Patients
Obesity is epidemic in the United States and a growing health issue worldwide. Estimates show that more than 78% of the adult U.S. population is either overweight, obese, or extremely obese [1,75]. While the proportion of the population categorized as overweight has remained essentially static since 1960, the numbers of obese and extremely obese have increased by 65% and 170%, respectively, in just the last two decades [1]. The trend is evident in all ages and geographic regions irrespective of ethnicity or socioeconomic status [120].
Although genetic and hormonal factors play a role, the foremost causes of the obesity epidemic are unhealthy eating habits and lack of work-based and/or leisure-time physical activity. According to data published by the Centers for Disease Control and Prevention (CDC), approximately half of U.S. adults do not perform the minimum amount of exercise needed to help maintain a healthy weight and prevent diseases such as diabetes and high blood pressure; 26% of adults do not perform any exercise at all [2]. This is despite the fact that the benefits of exercise are well-documented, including reducing the risk of heart disease, improving glycemic control in diabetes, improving blood pressure, alleviating depression, and generally preventing morbidity and mortality. Americans are also not making ideal nutritional choices. In 2015, only about 10% of adults and 6% of high school students met nutritional guidelines for fruit and vegetable consumption [3,4].
Compounding this problem, studies have found that less than 30% of overweight patients and approximately 40% of obese patients reported ever receiving advice from their physician to increase their physical activity or reduce their weight [41,100]. Even when physicians do give advice, too often they simply admonish patients to exercise, which has been shown to have little, if any, effect. Of the 30% who did receive advice in one study, only 38% received help in formulating a specific activity plan and only 42% received follow-up support [41].
Although obesity has been shown to be a risk factor for numerous diseases, such as diabetes, coronary artery disease, and sleep apnea, most overweight and obese people do not consider themselves at higher risk for medical problems or premature death. News stories on various diets have caused confusion among many patients and health providers, leading to frustration and subsequent inaction. However, patients generally want to receive information on weight reduction strategies. In a study asking patients to respond to the statement, "If my doctor advised me to exercise, I would follow his/her advice," more than 90% of respondents agreed with the statement [73].
Numerous treatments for obesity exist. The cornerstone of any treatment regimen includes behavioral modification, focusing on diet changes and exercise regimens. Additional therapies include pharmaceuticals, which can help sustain weight loss, as well as surgical therapies for those patients whose weight is causing significant health problems. Physicians and other healthcare professionals should recognize that recidivism and failure is quite high with all these therapies, and successful treatment will require a concerted effort on the part of physicians and other providers.
The following case study will be referenced throughout the text to illustrate the challenges of treating overweight/obese patients:
Patient B is a White woman, 52 years of age, with a history of type 2 diabetes mellitus, arthritis, hypertension, and hyperlipidemia who presents for a new patient evaluation. She is 5'2" and weighs 150 lbs. She is currently taking metformin, simvastatin, lisinopril, and celecoxib. On exam, her blood pressure is 150/92 mm Hg; heart rate 84 beats per minute; and respiration 16 breaths per minute. Laboratory analysis demonstrates blood glucose of 140 mg/dL; glycosylated hemoglobin 9.5%; cholesterol 205 mg/dL; low-density lipoprotein (LDL) 115 mg/dL; high-density lipoprotein (HDL) 52 mg/dL; and triglycerides 190 mg/dL. She asks for help in trying to lose weight. She expresses difficulty managing her weight since adolescence and has repeatedly cycled up and down with various fad diets and exercise programs. The patient states that she does not presently exercise because of arthritis in her knees and is confused about what she should or should not be eating. She wants to know if her weight really matters, because she knows plenty of people who are heavier than she and they seem to be fine. If it does matter, she wants to know what she should be doing.
The definition of obesity has been evolving over the past few decades. Historically, obesity has been defined simply as an excess of body fat [9]. Today, however, measurement of body weight and height is most often utilized as a measure of obesity.
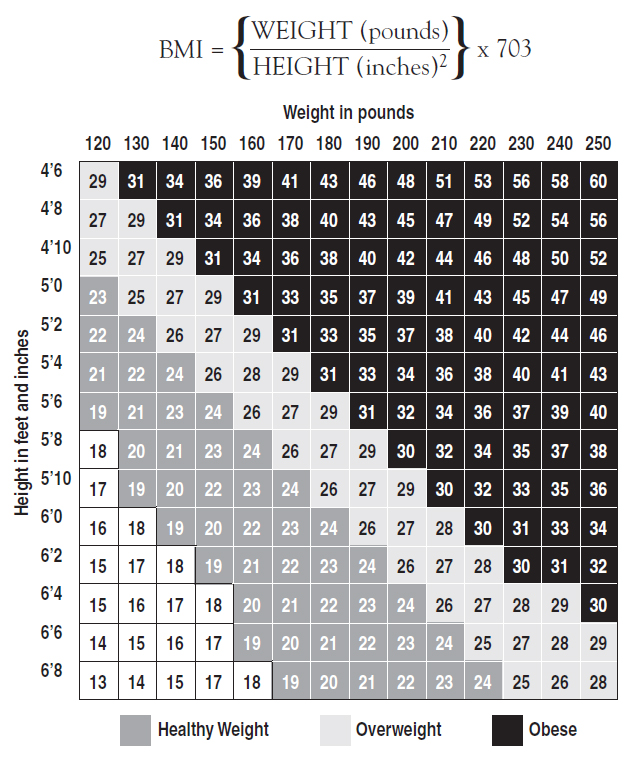
Initially, weight-for-height tables were used to determine the normal weight range for a given height. These tables were replaced with other indices when they were found to be of limited value due to their general estimates of frame size and bias toward the White population [10]. These tables were replaced with the body mass index (BMI), which is calculated by weight in kg/height in meters2 or [weight (lbs)/height (inches)2] x 703. For most individuals, BMI correlates well with the proportion of body fat.
BMI is considered the general standard for defining obesity (Figure 1). An online BMI calculator is available at https://www.nhlbi.nih.gov/health/educational/lose_wt/BMI/bmicalc.htm.
In 1990, the U.S. Department of Health and Human Services' Dietary Guidelines for Americans defined overweight as a BMI of at least 27 and obesity as a BMI of at least 30. Eight years later, the National Heart, Lung, and Blood Institute (NHLBI) of the National Institutes of Health (NIH) released guidelines that lowered the cutoff for overweight to a BMI of 25 but maintained the definition of obesity as a BMI of at least 30 [11]. (Note: Roughly, a BMI >25 corresponds to about 10% over one's ideal weight; a BMI >30 typically is an excess of 30 lbs for most people. These are rough estimates.) The term extreme (or morbid) obesity refers to obesity with a BMI greater than or equal to 40. These final definitions are consistent with definitions used by other national and international organizations, such as the World Health Organization (WHO). Table 1 illustrates the similarities in the classifications used by the WHO and the NHLBI.
BODY MASS INDEX CLASSIFICATION
| WHO Classification | BMI (kg/m2) |
|---|---|
| Underweight | <18.5 |
| Normal | 18.5–24.9 |
| Preobese | 25.0–29.9 |
| Obese Class I | 30.0–34.9 |
| Obese Class II | 35.0–39.9 |
| Obese Class III | >40.0 |
| The additional classification of obesity (Class I–III) was used to determine if the prevalence rate for comorbidities vary with class range. In addition, the BMI classification used 5 BMI unit intervals to classify obesity rather than using a single cut-off value. | |
These definitions are based on epidemiologic evidence that suggests health risks are greater at or above a BMI of 25, compared to those below 25. The risk of death from all causes rises with increasing BMI, with a significant increase at BMI greater than 30. In a large cohort study published in the New England Journal of Medicine in 2006, persons with a BMI greater than 30 had mortality rates two to three times that of persons with BMI between 20 and 25 [12].
The U.S. Preventive Services Task Force (USPSTF) recommends that clinicians offer or refer patients with a BMI of 30 or greater intensive, multicomponent behavioral interventions.
(https://jamanetwork.com/journals/jama/fullarticle/2702878 Last Accessed: January 18, 2024)Strength of Recommendation: B (The USPSTF strongly recommends that clinicians routinely screen eligible patients. The USPSTF found good evidence that obesity screening improves important health outcomes and concludes that benefits substantially outweigh harms.)
BMI does have limitations as a measurement of overweight and obesity. Although BMI provides a more accurate measure of total body fat compared with body weight alone, it can be misinterpreted in some circumstances. For instance, a muscled athlete would be considered overweight if BMI were used alone, despite his or her very low fat content. BMI can also underestimate body fat in persons who have lost muscle mass, such as elderly patients. Therefore, using other estimates, such as the triceps skinfold test, in addition to BMI may provide a better estimate of a patient's weight-related health status, especially in some atypical patients. (Note: There are various anatomic sites around the body that may be used for the triceps skinfold test, other than the triceps. The tester pinches the skin, raising only a double layer of skin and the underlying adipose tissue. The calipers are then applied 1 cm below and perpendicular to the pinch. Three readings are taken and then averaged to produce a final reading that is used in an equation to provide a more accurate estimate of body fat.) As a general reference, the U.S. Department of Defense states that the maximum allowable percent body fat of military personnel is 26% for men and 36% for women [13].
In defining obesity, NIH also identified excess fat in the abdomen out of proportion to total body fat as an independent predictor of risk factors and morbidity [11]. The gender-specific cutoffs for waist circumference are as follows:
Men: >40 inches (102 cm)
Women: >35 inches (88 cm)
These are of value only for those with a BMI between 25.5 and 34.9. It is not useful to measure waist circumference in individuals with BMI >35, as such patients are already at increased risk.
In this example, Patient B's BMI is 27. Her waist circumference is 35.5 inches. Both of these measurements place her at increased risk for morbidity and death. Intervention should be made.
According to the WHO global estimates, worldwide obesity has tripled since 1975. During the period 2016–2020, more than 1.9 billion adults 18 years and older (39% of the world's population) were overweight; of these, 650 million (13%) were obese [116]. Overall, about 13% of the world's adult population (11% of men and 15% of women) were obese in 2016. In 2019, an estimated 38 million children younger than 5 years of age were overweight or obese, which is 24% greater than in the year 2000. Among children and adolescents 5 to 19 years of age, 360 million were overweight or obese in 2016. an increase in prevalence from 4% in 1975 to just over 18% in 2016 [116].
Since 1960, the prevalence of obesity in the United States has been on an upward trajectory, with rates increasing dramatically in the past few decades. In 1980, the percentage of obese and extremely obese adults was 15% and 1.4% of the total population, respectively; by 1994, the numbers had increased to 23.2% and 3.0% [1]. In the year 2000, 30.9% of the adult population was obese and 5.0% were extremely obese [1]. Data collected in 2017–2020 show that 41.9% are obese and 9.2% are extremely obese (class III); an additional 31.9% of adults are overweight [1,75]. That means that more than 83% of Americans 20 years of age or older are above a healthy weight and are at an increased risk for disease and early death.
With race/ethnic origin not factored, the prevalences of overweight and obesity are higher for men (38.2% and 43.0%) than for women (25.8% and 41.9%), but rate of extreme obesity is higher among women [75]. In the overall population, approximately 6.9% of men and 11.5% of women are extremely obese [1,75].
When considered as a single race, the prevalence of obesity is greater among individuals of African (49.9%) and among individuals of Hispanic (45.6%) descent than among adults of European or Caucasian descent (41.4%) [75]. Native American/Alaska Natives and Native Hawaiian/Pacific Islanders have an obesity prevalence of 43.7% and 34.6%, respectively [42,74]. Asian Americans are an exception, with a prevalence of 17.4%, much lower than in the general population. Although the rate of obesity is higher in many American racial/ethnic groups compared with non-Hispanic White population, White individuals make up the majority of cases [75].
Obesity is most common among individuals 40 to 59 years of age, with 44.8% of American men and women in this age group fitting this description [42,75]. However, roughly 57.5% of African American women and 51.1% of Hispanic women in this age group are obese [42,75]. There is also a higher incidence of obesity (greater in women than in men) with lower socioeconomic status among all races [42,74].
Of particular concern is the increase in the number of children who have high BMIs. Presently, nearly 13% of children 2 to 5 years of age, 20.7% of children 6 to 11 years of age, and 22.2% of adolescents between 12 to 19 years of age are obese [14,110]. Hispanics (26.2%) and non-Hispanic Black individuals (24.8%) have a higher prevalence of obesity than non-Hispanic White individuals (16.6%). The prevalence of obesity in adolescents has more than tripled since 1970 [14]. This is especially troubling because overweight adolescents have a 70% chance of becoming overweight or obese adults; if their parents are overweight or obese, this chance increases to 80% [101]. Adolescent obesity is associated with increased risk for cardiovascular disease, type 2 diabetes, and certain malignancies (e.g., leukemia, Hodgkin lymphoma, colorectal cancer, breast cancer) in adulthood [121].
The impact of obesity on general health is significant. A BMI of 35 or greater increases mortality 40% for women and 62% for men, and obesity in general results in an estimated 100,000 to 300,000 preventable deaths per year [7,8]. Preventable deaths attributable to poor diet and inactivity are second only to deaths due to tobacco use, but as cigarette smoking has declined, preventable deaths attributable to obesity-related conditions are set to overtake tobacco-related deaths [76].
The economic costs are significant as well, with the total annual costs of obesity estimated to be $173 billion [5,16,122]. Roughly 10% of the nation's healthcare expenses are obesity-related, and this is expected to increase to between 16% and 18% by 2030 [5,102]. In addition, obese patients have a 46% increase in inpatient costs, 27% increase in physician visit and outpatient costs, and spend 80% more on prescription drugs than those with normal BMIs [112].
As noted, although the impact of obesity on general health has become highly publicized, most overweight Americans do not consider themselves at higher risk for medical problems or premature death. According to the results of a survey conducted by Shape Up America, 7 out of 10 overweight respondents said that their excess pounds were not a health concern. However, the survey results indicated that approximately 33% of the respondents had already developed a weight-related medical condition [54]. Despite the evidence linking obesity and poor health, many Americans still consider excess weight to be only a cosmetic issue. This is in light of the fact that more than 80% of patients with diabetes are overweight or obese [12].
One of the most common, but oversimplified, explanations for obesity is that it is merely the result of sustained caloric imbalance. Caloric imbalance can be caused by either excessive intake of energy or decreased energy expenditure. With the increased availability of foods with poor nutrition content and decreasing desire for an active lifestyle, the resulting obesity is unsurprising. The cultural evolutionary explanation of obesity argues that our species evolved in an environment where food was often scarce, so our bodies developed an "evolutionary predisposition to store energy in the form of fat" in preparation for those shortages [18].
Though the scientific community has been unable to identify a single etiologic agent for obesity, there have been clinical advances in the past two decades. Obesity is known to be associated with certain exogenous causes. Genetic factors gained national attention after the discovery of leptin in 1995 by positional cloning in the leptin-deficient mouse model of obesity [19]. Leptin (derived from the Greek word leptos, meaning "thin") is a 16-kilodalton adipocyte-derived hormone from the ob gene and has been the focus of many genetic investigations to elucidate the pathophysiology of obesity. Though this finding is relatively recent, its existence was suspected twenty years ago. In 1978, Coleman proposed that a circulating factor in the plasma of the db mouse strain, which is both diabetic and obese, could reduce the obesity of the ob mouse (a strain of mice with mutations in leptin) [20]. The db mice were found to have mutations in the leptin receptor and were subsequently resistant to the leptin, unlike the ob mice who possessed a mutated leptin gene but functional leptin receptors. Further investigations revealed that injections of leptin in ob mice could cure obesity and diabetes. After locating the human homologues to the leptin gene and its receptor in 1999, the chromosomal locus containing the leptin gene was determined to be genetically related to human body weight [21]. However, only a few people with mutated leptin genes have been identified, while the majority of obese patients have fully functional leptin genes and receptors.
Genetic diseases with associated obesity include Schinzel syndrome, Bardet-Biedel syndrome, Albright hereditary osteodystrophy, and Prader-Willi syndrome. Many of these genetic disorders present with dysmorphic features, developmental delay, and obesity in addition to changes seen specifically with each disorder [22]. For instance, young males with Prader-Willi syndrome present with the features described above as well as with linear growth defects and undescended testicles.
Overall, the relationship between genetics and obesity cannot be fully determined at this time. Evidence suggests a link between the two, implying that genetics is one of the complex factors involved in the development of this prevalent condition. Although many argue that "obesity genes" cannot be responsible for the epidemic, because the gene pool in the United States had not changed significantly between 1980 and 1994, the etiology of obesity is most likely multifactorial [23]. In 2010, one group of researchers confirmed 14 genetic variations and discovered an additional 18 variations associated with obesity [77]. In 2015, the group published additional research that identified a total of 97 genetic variations [111]. Although the progress with genetic variations related to BMI is promising, further research is needed to clarify the influence of genetics.
Biologic factors must also be considered. Proteins and receptors appear to have a role in weight control. For example, orexin A and B are located in the lateral hypothalamus, an area which may regulate body weight. Ongoing research may help determine the role of orexin in obesity.
Environmental factors seem to play a significant role as well. Data from a longitudinal twin-family study and co-twin control studies combined with population-based data on patterns of dietary intake and physical activity provide some evidence that environment can contribute to obesity [74]. Environmental factors include technologic advances in food processing, marketing, advertising, and behavioral lifestyle. Some theorize that obesity is self-fulfilling in that if an individual is told they are predisposed to becoming fat, he or she will decide there is no point in eating healthy or exercising [78].
Occasionally, obesity is due to endocrinologic origins from hypothyroidism or Cushing syndrome. However, both of these conditions, along with other diseases associated with obesity, present with additional signs and symptoms. Moreover, they typically have appropriate treatment regimens that address the underlying cause of the obesity.
Given the influence of genetic and environmental factors, the issue of obesity cannot be simplified to sustained caloric imbalance. There are complex metabolic, psychologic, endocrinologic, social, and cultural influences regulating energy intake and energy expenditure, which indicates that obesity is more than a lack of self-control when presented with food.
Obesity is associated with large number of major medical concerns, such as elevated serum triglycerides (>200 mg/dL), and is a risk factor for many diseases, including [24,80,81,112]:
Sleep apnea
Stroke
Dementia
Hypertension
Dyslipidemia
Coronary heart disease
Type 2 diabetes
Osteoarthritis
Colon, breast, endometrial, and possibly other cancers
Gallbladder disease
Stress incontinence
Amenorrhea/menorrhagia
There is evidence that excess body weight is associated with increased risk for a range of malignancies: endometrial, esophageal, renal, pancreatic, and hepatocellular carcinomas and colorectal, postmenopausal breast, ovarian, gallbladder, and thyroid cancers [123]. In the Nurses' Health Study (a large prospective cohort study involving more than 100,000 women), women older than 35 years with a BMI greater than 27 were found to have an increased risk for cancer, heart disease, and other diseases. For instance, women gaining more than 20 pounds (9 kg) between 18 and 35 years of age doubled their risk for breast cancer compared with women who maintained their weight [25]. Additionally, the age and smoking-adjusted relative risk of non-fatal myocardial infarction and fatal coronary disease for women with BMI 25 to 29 was 1.8; for women with BMI greater than 29, it was 3.3.
Left ventricular hypertrophy (LVH) is often seen in obese patients and correlates to the resulting systemic hypertension [26]. The risk for type 2 diabetes has been reported to be twofold in the mildly obese, fivefold in moderately obese, and tenfold in extremely obese persons [27].
In one study, individuals with a BMI of at least 30 had an elevated risk of pancreatic cancer compared to those with a BMI of less than 23 [28]. A study published in 2012 involving 720,000 men found that overweight adolescents had more than double the risk of developing pancreatic cancer as young or middle-age adults compared to normal weight individuals [79]. In general, obese patients showed an increased risk of 5.4 times that of non-obese patients for endometrial cancer, 3.6 times for gallbladder cancer, 2.4 times for cervical cancer, 1.6 times for ovarian cancer, 1.5 times for breast cancer, 1.7 times for colorectal cancer, and 1.3 times for prostate cancer [29]. Cancer mortality is also increased in obese patients.
The term "metabolic syndrome" has been used when three or more of the following risk factors are present:
Abdominal obesity: waist circumference >40 inches in men or >35 inches in women
BMI >25
Triglycerides >150 mg/dL
HDL <40 mg/dL in men, <50 mg/dL in women
Blood pressure >130/>85 mm Hg
Fasting glucose >110 mg/dL or two-hour post glucose challenge >140 mg/dL
The development of this metabolic disorder is promoted by excess body fat and physical inactivity. It is believed to predispose patients to heart disease, cerebrovascular disease, and diabetes due to the associated dyslipidemia, hypertension, glucose intolerance, and hypercoagulability. Reduction in body weight and body fat through exercise also improves glycemic control and reduces the complications of diabetes [82].
Obesity, with or without components of the metabolic syndrome, is a risk factor for an increasingly common form of heart failure with preserved ejection fraction (EF >50%), characterized clinically by dyspnea and overt or absent signs of cardiac decompensation. Approximately 65% of patients with this form of heart disease present with dyspnea and physical examination, radiographic, or echocardiographic evidence of heart failure, as well as overt signs of volume overload at rest; about 35% of patients present with unexplained dyspnea and have no clear physical exam, radiographic, or echocardiographic signs of heart failure [15]. Patients without overt signs of heart failure exhibit elevated atrial pressures with exercise by hemodynamic stress testing or Doppler echocardiography. The condition is designated heart failure with preserved ejection fraction.; It affects approximately 3 million persons in the United States and has an annual mortality of 15% [15]. Evidence suggests that adipose tissue itself contributes to the development, progression, and onset of adverse outcomes in obese patients with heart failure with preserved ejection fraction. Visceral adiposity is associated with increased inflammation, left ventricular hypertrophy, insulin resistance, and both diastolic and systolic left ventricular dysfunction [106]. Heart failure with preserved ejection fraction is managed with pharmacotherapies combined with diet-induced weight loss, which has been shown in clinical trials to independently improve functional status and quality of life [15,106].
One can stratify overweight and obese patients to determine their absolute risk by incorporating the presence of comorbidities and cardiovascular disease risk factors. Patients with coronary heart disease, other atherosclerotic diseases, type 2 diabetes, and sleep apnea are at "very high risk" for death; in comparison, those with three or more cardiovascular risk factors are at the "highest absolute risk." (Note: These risk factors include hypertension, hypercholesterolemia, smoking, family history of early heart disease, and age [men older than 45 years of age, women older than 55 years of age].)
During the coronavirus disease (COVID-19) pandemic in the United States, obesity emerged as an independent risk factor for severe COVID-19, especially among adult patients younger than 60 years of age. Multiple reports, ranging from single-center studies to analyses of records from large patient care networks, consistently found that severe obesity (body mass index >35) was associated with higher rates of hospitalization, respiratory failure, and mortality from COVID-19 [124,125]. The risk varies with degree of obesity and is independent of obesity-associated comorbidities. The impact is more striking among men with COVID-19 than women. There are multiple mechanisms by which obesity may contribute to adverse outcomes in patients with COVID-19. In addition to obstructive pulmonary physiology with sleep apnea, severe obesity leads to immune dysfunction, depression of anti-inflammatory signaling, increased pro-inflammatory signaling, and alterations in vascular endothelium that worsen lung inflammation and alveolar damage [124].
Conditions that are associated with obesity usually worsen as the degree of obesity increases. For instance, one study showed that the risk of developing dementia increases 3.6 times in individuals with high BMIs (particularly in individuals with both high BMI and abdominal obesity) [81]. Moreover, individuals' health typically improves and risk factors lessen as obesity is successfully treated. In addition, overweight and obese patients often suffer from emotional distress and face discrimination in their personal and professional lives. Many overweight patients suffer from social stigmatization and isolation, which subsequently increases morbidity and mortality. In one study, 13% of all women reported delaying or canceling a doctor's appointment because of concerns about their weight (e.g., embarrassment, fear of a lecture), while 32% of those with BMI greater than 27 and 55% with BMI greater than 35 had done the same [30].
Patient B has several comorbidities, including diabetes, dyslipidemia, hypertension, and osteoarthritis. She is at "very high risk" for premature death. Most of these conditions would improve if her weight were reduced.
The goal of therapy is to reduce body weight as well as body fat and maintain a lower body weight for the long term. The rate of weight loss should be 1 to 2 lbs per week, with a goal of 10% weight loss over six months. Moderate weight loss, defined as 5% to 10% reduction in baseline weight, is associated with clinically meaningful improvement in obesity-related metabolic risk factors and comorbidities, including improved pancreatic beta-cell function, increased sensitivity of liver and skeletal muscle to insulin, and significant reductions in systolic and diastolic blood pressure [126]. It is important to note that weight loss as modest as 10 lbs reduces the risk factors for several diseases. Such weight loss can lower blood pressure, lower blood sugar, reduce inflammation, and improve lipid levels. Unfortunately, most patients believe a weight loss of 30 to 40 lbs is necessary to medically benefit and become discouraged when they do not see such results [31]. Patients should set realistic expectations from the start, with the idea that small losses of 10 lbs can be considered successes. Moreover, physicians must emphasize the importance of long-term weight management and weight loss rather than short-term extreme weight reduction.
For high-risk obese persons, sustained moderate weight loss aids in prevention of disease and larger relative weight reductions may lead to disease resolution, Obese patients with impaired glucose tolerance who received an intensive lifestyle intervention had a mean weight loss of 5.6 kg at 2.8 years and a 58% relative reduction in the risk of type 2 diabetes [126]. In a study comparing lifestyle intervention with bariatric surgery for management of obese patients (BMI 30 to 40) with type 2 diabetes, the mean reduction in body weight at three years was 25% for patients randomized to Roux-en-Y gastric bypass, and 40% of patients in this cohort experienced complete or partial remission of diabetes [127].
Of note, weight reduction treatment is not recommended for pregnant women or for patients with unstable mental or medical conditions. Patients with terminal illness may also be excluded from treatment.
Before any treatment plan is attempted, one must assess the patient's willingness and motivation. If a patient is not willing to attempt weight loss, despite the risks as well as existence of current medical problems, treatment will be unsuccessful. Patients cannot be forced to lose weight, nor can they be berated or shamed into doing it. A productive dialogue focusing on the patient's goals and the health risks of being overweight will be the most successful.
In 2000, the National Institutes of Health (NIH) released guidelines for identification, evaluation, and treatment of obesity [69]. In this guideline, a 10-step treatment approach was presented. Expanding on these guidelines, in 2013, the American Heart Association (AHA) and American College of Cardiology (ACC) released an evidence-based, peer-reviewed guideline for the management of overweight and obesity in adults [112]. In these guidelines, the AHA and the ACC recommended that obesity be classified as a disease and devised a treatment plan using a chronic diagnosis management model. Both will be discussed in further detail in this course.
Patient B clearly is seeking guidance. She is interested in a treatment plan and illustrates this by seeking additional information despite her failure at past attempts. She must realize that her weight really does matter and indeed is already contributing to her morbidity. Her medical conditions are stable. She is eligible and ready for treatment.
The 10-step approach, as shown in Table 2, is recommended by the NIH in developing an assessment and treatment plan.
TEN STEPS TO ASSESSING/TREATING OVERWEIGHT AND OBESITY IN THE PRIMARY CARE SETTING
|
The goal of the 2013 guideline published by the AHA/ACC was to, using an evidence-based approach, increase the quality and rigor of the overweight and obesity treatment guidelines, and to assist primary care physicians to more aggressively diagnose and treat obesity as a disease. The guideline consists of a review of assessment methods and treatment modalities that incorporate the steps recommended by the NIH in Table 2, but also includes a comprehensive algorithm that guides primary care physicians through specific steps, and references expanded sections describing the process that should be used to proceed with treatment [112]. The complete guideline with evidence-based findings, including algorithm, is available at https://www.ahajournals.org/doi/full/10.1161/01.cir.0000437739.71477.ee.
The treatment of obesity includes three types of therapies:
Behavioral
Pharmacologic
Surgical
Behavioral therapy includes a combination of diet and exercise and is the cornerstone of any weight reduction treatment. Diet and exercise remain a significant challenge for most adults, as evidenced by the number of overweight and obese people. Most adults do not eat nutritiously and do not exercise regularly. About 26% of adults report engaging in no physical activity at all in the past month [2]. NHIS data show nearly 47% of adults meeting neither aerobic nor muscle-strengthening activity recommendations, with only about 20% of adults meeting these guidelines [32].
Reviewing and modifying diet is one of the most important steps in helping patients lose weight. As a simple rule, caloric intake should be reduced by 500–1,000 calories per day from a patient's current level. Patients with a BMI of 27–35 should reduce total calories by 300–500 daily; patients with BMI greater than 35 should reduce total calories by 500–1,000 daily. This reduction will produce the recommended weight loss of 1 to 2 lbs per week in most patients. The recommended number of total calories will vary depending upon activity level: 1,600 calories for most sedentary women, 2,200 calories for sedentary men or active women, 2,600 calories for active men. To calculate specific caloric requirements, the following approach is useful:
First calculate resting energy expenditure (REE)
For men: (10 x weight (kg)) + (6.25 x height (cm)) - (5 x age + 5)
For women: (10 x weight (kg)) + (6.25 x height (cm)) - (5 x age - 161)
Multiply REE by activity factor (AF).
For light activity, AF is 1.5 for women, 1.6 for men. For high activity, AF is 1.6 for women, 1.7 for men.
In terms of diet specifics, conflicting information exists. Many newspapers and magazines offer detailed articles addressing the successes of individual patients on the Atkins diet, the Ornish plan, the Zone diet, the Body-for-Life program, and others (Table 3). Differences among these diets leave patients confused and discouraged. The Internet compounds the confusion by providing unfiltered information and a lack of emphasis on current research and evidence-based medicine.
VARIOUS POPULAR DIETS
| Diet Plan | Breakdown | Mechanism of Action | ||
|---|---|---|---|---|
| Atkins/Ketogenic | High fat (55% to 65%) Low carbs (<100 g/day) | Reducing carbohydrates causes ketosis, which induces use of excess body fat for fuel | ||
| Ornish |
| Reduction in total calories and total fat | ||
| Zone | 40% carbs, 30% protein, 30% fat | Reduction in total calories causes weight loss | ||
| Body-for-Life | High protein, moderate carbs, low fat, all eaten at same time, with small, frequent meals | More steady release of insulin causes less fat deposition |
There has been some progress in assessing these various diets, but without strong evidence in favor of any particular one. In 2003, a study conducted at the University of Pennsylvania, supported by the NIH, concluded that the Atkins diet resulted in greater weight loss (approximately 4%) at the end of one year, as well as an improvement in some cardiovascular risk factors [33]. In 2005, researchers at Tufts University compared the Atkins, Ornish, Weight Watchers and Zone diets, with weight reduction and cardiovascular disease reduction as outcomes. (The Atkins diet restricts carbohydrates, the Zone diet involves balancing macronutrient intake, the Ornish diet restricts fat, and the Weight Watchers diet restricts calories.) After one year, all diets produced moderate weight loss and improvement in HDL, C-reactive protein, and insulin levels. Increased adherence to each diet was associated with increased weight loss, but overall adherence was low [34]. In 2007, researchers reported on a randomized trial of the Zone, Atkins, Ornish, and LEARN diets in 311 overweight or obese non-diabetic, premenopausal women. (The LEARN diet is based on national nutrition guidelines.) Again, all diets provided modest weight loss at one year. The Atkins diet produced the most weight loss, with improvements in cardiovascular risk factors that were comparable to or better than the other diets. However, weight loss trajectories had not stabilized at the end of the study, suggesting that longer observation might produce different outcomes [35]. In 2014, researchers compiled information from 48 randomized trials regarding the effectiveness of named diet plans, including Atkins, Ornish, Zone, and others. It was found that significant weight loss occurred with any of the diets, with minimal differences between the amount of weight lost at 6- and 12-month follow-up. The researchers concluded that, of the diets reviewed, any diet that an individual will able to adhere to should be recommended for weight loss [113]. While information on specific diets is becoming more consistent, for each diet plan, larger and longer studies are necessary to assess long-term benefits and risks.
It is important that any diet contain food from all food groups, so that it remains nutritionally adequate. "Fad diets" typically have nutritional deficiencies, and this is one reason why they are potentially dangerous. For example, high-fat, low-carbohydrate diets are low in vitamins E and A, thiamin, folate, calcium, magnesium, and zinc. Low-fat diets are typically deficient in vitamin B12.
Instead of recommending a specific type of diet, physicians should encourage patients to focus on well-balanced meals from the various food groups. Recommendations from the Institute of Medicine provide a useful framework, as do the Dietary Guidelines for Americans.
In 2005, the Institute of Medicine (IOM) issued its first volume in a series of reports that suggest dietary reference values for intake of nutrients. This project was released by the Standing Committee on the Scientific Evaluation of Dietary Reference Intakes of the Food and Nutrition Board from the IOM, a division of the National Academies. The report establishes the Dietary Reference Intakes (DRIs) for energy and macronutrients: carbohydrates, fiber, fat, fatty acids, cholesterol, protein, and amino acids. A synopsis of the main findings follows. The full report, with the detailed rationale used to establish each guideline/recommendation, can be accessed online at https://www.nap.edu/read/10490/chapter/1.
The following ranges are recommended for percentage of daily caloric intake [36]:
Carbohydrates: 45% to 65%
Sugars: 25%
Fats: 20% to 35%
Protein: 10% to 35% (dietary protein should be 0.8 g/kg/day)
Fiber:
Men younger than 50 years of age: 38 grams per day
Women younger than 50 years of age: 25 grams per day
Men older than 50 years of age: 30 grams per day
Women older than 50 years of age: 21 grams per day
The report distinguishes the different types of fat. Saturated fat and trans fatty acids typically raise the amount of LDL in the bloodstream. Because this type of fat has little value, there is no recommended intake requirement, and people should be advised to keep consumption as low as possible. Sources include meat, poultry, baked goods, and dairy products, as well as some vegetable sources, such as coconut and palm oils.
In contrast to saturated fat, monounsaturated and polyunsaturated fat reduce blood cholesterol levels. As much as possible, one should replace saturated fat with unsaturated fat. Two types of polyunsaturated fat are critical elements of a healthy diet because they are not synthesized in the body. These are omega-3 and omega-6. Omega-3, or alpha-linolenic acid, consumption should be 1.6 g for men and 1.1 g for women; omega-6, or linoleic acid, consumption should be 17 g for men and 12 g for women daily. Sources of monounsaturated fat include plants, peanuts, avocado, and canola oil. Sources of polyunsaturated fat include safflower, sunflower, corn, and soybean oils. Omega-3 fatty acids are found in oily fish and flaxseed.
An interactive dietary reference intake calculator is available at https://www.nal.usda.gov/human-nutrition-and-food-safety/dri-calculator. Height, weight, age, and activity level are inputted into the calculator, and a complete individualized profile of caloric needs—plus vitamin, mineral, and water intake—is outputted for the patient.
The 2020–2025 Dietary Guidelines for Americans recommends a healthy eating pattern to "help people achieve and maintain good health and reduce the risk of chronic diseases throughout all stages of the lifespan" [70]. Decreased caloric intake with increased exercise is suggested for people who need to lose weight, with the goal of slow and steady weight loss over time. The 2020–2025 Dietary Guidelines for Americans features four new overarching guidelines that provide a flexible framework for encouraging individuals and other areas of society to assist in making healthier food choices throughout life. These guidelines use a social-ecologic model for food and physical activity choices that acknowledge individual preference, cultural differences, traditional food choices, and individual budget. The four overarching guidelines are [70]:
Follow a healthy dietary pattern at every life stage. At every life stage—infancy, toddlerhood, childhood, adolescence, adulthood, pregnancy, lactation, and older adulthood—it is never too early or too late to eat healthfully.
Customize and enjoy nutrient-dense food and beverage choices to reflect personal preferences, cultural traditions, and budgetary considerations. A healthy dietary pattern can benefit all individuals regardless of age, race, or ethnicity, or current health status. The Dietary Guidelines provides a framework intended to be customized to individual needs and preferences, as well as the foodways of the diverse cultures in the United States.
Focus on meeting food group needs with nutrient-dense foods and beverages, and stay within calorie limits. An underlying premise of the Dietary Guidelines is that nutritional needs should be met primarily from foods and beverages—specifically, nutrient-dense foods and beverages.
Limit foods and beverages higher in added sugars, saturated fat, and sodium, and limit alcoholic beverages. At every life stage, meeting food group recommendations, even with nutrient-dense choices, requires most of a person's daily calorie needs and sodium limits. A healthy dietary pattern doesn't have much room for extra added sugars, saturated fat, or sodium or for alcoholic beverages.
Specific recommendations for adults, based on a "reference diet" of 2,000 calories per day, include [70]:
Two cups of fruit and 2½ cups of vegetables per day, with an emphasis on high-fiber choices; weekly recommendations are 1½ cups/week of dark green vegetables, 5½ cups/week of red/orange vegetables, 1½ cups/week of beans/lentils/peas, 5 cups/week of starchy vegetables, and 4 cups/week of other vegetables
Six ounce-equivalent of grains, with at least half of all grain products consumed coming from whole grains
3 cups per day of fat-free or low-fat milk or equivalent dairy products
5½ ounces of protein/day, including 8 ounces of seafood per week; 26 ounces of meat, poultry, and eggs per week; and 5 ounces of nuts, seeds, and soy products
12 g of oils per day, with a focus on healthy oil choices
Less than 12% of calories from other uses, including alcohol, saturated fats, and added sugars
Less than 2,300 mg (approximately 1 tsp of salt) of sodium per day for individuals 14 years of age and older
The USDA's MyPlate plan and the DASH diet both fulfill the Guidelines' recommendations. MyPlate is an individualized guide for healthy eating based on age, sex, height, weight, and physical activity level. Patients can create their own MyPlate plans at https://www.myplate.gov. The DASH diet (Dietary Approaches to Stop Hypertension) was originally developed as a method to prevent and treat hypertension, but it provides a balanced diet that is appropriate for most adults. Patient-friendly information about the DASH diet is available at https://www.nhlbi.nih.gov/health-topics/dash-eating-plan.
Patients must keep in mind that as they change their diet and begin to lose body weight, body fat and lean body mass also decrease. The optimal goal of therapy is to maximize loss of body fat and minimize loss of lean body mass.
Exercise increases energy expenditure, and regular physical exercise is an important predictor of long-term weight maintenance. It is as important as diet, and patients should understand this point. Several studies have shown that patients who diet and exercise regularly are much more likely to maintain weight loss than those who simply change their diet. Multiple studies have demonstrated that a program of diet and exercise can reduce the number of persons who progress from impaired glucose tolerance to frank diabetes by 50% or more [37,38,39,40].
As noted earlier, approximately 26% of American adults rarely (or never) exercise [2]. There are numerous reasons for this, including lack of interest, competing demands for leisure time, lack of knowledge of proper technique, and fear of injury. Compounding this problem, in a 2001 survey, it was found that only 28% of subjects reported receiving advice from their physicians to increase their physical activity [41]. Of the individuals who received advice, only 38% (or 11% total group) received help formulating a specific activity plan, and 42% received follow-up support. As noted, in 2013, the AHA/ACC published obesity guidelines that specifically detail how primary care physicians can incorporate assessment and treatment for overweight and obesity into daily practice [112]. The recommendation to consider obesity as a disease and provide an algorithm for assessment and treatment was made due to continued undertreatment noted during systematic reviews in 1998 and 2005 [69,112].
According to the CDC, adults should engage in at least 150 minutes of moderate-intensity aerobic activity (e.g., brisk walking) or 75 minutes/week of vigorous-intensity exercise (e.g., jogging, running) every week, combined with muscle-strengthening activities that work all major muscle groups (legs, hips, back, abdomen, chest, shoulders, and arms) two or more days per week for moderate health benefits [83]. (Note: A weekly workout can include a mix of exercise intensity equal to the given recommendations.) For increased health benefits, moderate-intensity aerobic exercise should be doubled to 300 minutes per week [83].
The 2020–2025 Dietary Guidelines for Americans include recommendations for physical activity similar to the CDC recommendations [70,83]. It should be emphasized that usual daily activities at work or around the house should not be counted towards patients' exercise goals, but that these should continue in addition to exercise. Adults require at least 150 to 300 minutes of moderate-intensity aerobic activity (e.g., brisk walking, fast dancing) each week. It is also recommended that adults engage in muscle-strengthening activity (e.g., lifting weights, push-ups) at least two days each week [70].
In 2007, the AHA released guidelines for physical activity, in partnership with the American College of Sports Medicine (ACSM) [43]. These guidelines are intended to clarify recommendations originally released in 1995 by the ACSM and the CDC. For healthy adults 18 to 65 years of age, the AHA and ACSM recommend:
Moderate-intensity aerobic activity on five days per week for 30 minutes or more, or vigorous-intensity aerobic activity on three days per week for 20 minutes or more.
Resistance or strength training, or activity that improves strength and endurance, at least twice a week.
Vigorous- and moderate-intensity activity can be combined to meet the goals. For example, a brisk half-hour walk twice a week plus a 20-minute jog twice a week fulfills the recommendations. Moderate-intensity bouts of exercise lasting at least ten minutes can be added together over the course of a day. Activities of daily living, such as household chores, do not count toward the goals.
Strength training should include 8 to 10 exercises using the major muscle groups on two or more non-consecutive days. Weights should allow 8 to 12 repetitions before fatigue.
The AHA and ACSM also offer specific recommendations for older adults [44]. Aerobic and strength training goals are the same, although the guidelines note that the same exercise may be "moderate" for some older adults and "vigorous" for others, depending on baseline fitness level. Additional recommendations include:
Exercises to promote flexibility, for at least 10 minutes two days a week.
Balance-improving exercises for adults at risk of falls.
Integration of preventive and therapeutic recommendations, so as to accommodate illness or restrictions on movement while avoiding a sedentary lifestyle.
The key is to make physical activity a part of everyday life by encouraging patients to choose activities of interest. Exercise should not be a chore, but rather an enjoyable activity that people look forward to. This may be light jogging, dancing, vigorous walking, or perhaps swimming for patients with arthritis. Patients should be encouraged to surround themselves with people supportive of exercise, who may join them in this activity. Patients should also consider varying their routine so they do not get bored. One study demonstrated that women older than 50 years of age who spent approximately 2.5 hours per week walking briskly reduced their risk of cardiovascular disease by 30% [45]. For patients with chronic renal insufficiency, resistance training has been shown to be effective against the catabolism of a low-protein diet and uremia [46].
It is also recommended that patients self-monitor. This entails keeping a diary of caloric intake and physical activity. Such a log encourages adherence, and most patients can see some success by noting their daily progress over time. They should bring this log to each visit, which should be one to two times per month early on. Physicians should review this diary with patients to ensure that they are properly following a structured program. Some patients will need closer monitoring, depending on cardiac risk and the presence of other medical conditions.
Although behavioral strategies can be effective, weight regain is common. Patients typically regain weight after leaving a structured program. Patients must understand that these changes must become their daily lives. They should change slowly, choosing foods and activities they can enjoy. They need to understand that occasional setbacks may occur, and that instead of becoming frustrated they should try to remain focused on long-term goals. Permanent lifestyle changes remain one of the most difficult interventions to implement. Patients need support, positive feedback, continual encouragement, and reinforcement.
Patient B should be counseled to adopt a diet and exercise regimen. She needs to decrease her calories by 500 calories per day and distribute her calories to 45% to 65% carbohydrates, 25% sugar or less, 20% to 35% fat, and 10% to 35% protein. She should choose an exercise program she enjoys—perhaps swimming, which would not only cause less stress on her joints but may also improve her arthritis. She should start slowly, 10 to 20 minutes several times a week, gradually building up to one hour, five or more times per week.
The Department of Veterans Affairs and the Department of Defense suggest offering prescribed pharmacotherapy (specifically liraglutide, naltrexone/bupropion, orlistat, or phentermine/topiramate) for long-term weight loss in patients with a BMI ≥30 and for those with a body mass index ≥27 who also have obesity-associated conditions, in conjunction with a comprehensive lifestyle intervention.
(https://www.healthquality.va.gov/guidelines/CD/obesity/VADoDObesityCPGFinal5087242020.pdf Last Accessed: January 18, 2024)Strength of Recommendation: Weak for
Pharmacotherapy should only be used as an adjunct to lifestyle modification, including calorie restriction and increased physical activity. It should not be used as a primary treatment option or by people who are unwilling to make behavioral changes. Rather, if lifestyle changes do not promote weight loss after six months, drugs should be considered. Most drugs are recommended for use in patients with a BMI >30 or in those with a BMI >27 and comorbidities such as type 2 diabetes, hypertension, or sleep apnea [128]. Many pharmacotherapies combined with exercise and lifestyle modification are effective in achieving meaningful weight reduction; the more elusive goal has been maintenance of healthy weight required to alleviate comorbidities (e.g., type 2 diabetes) and prevent potential complications (e.g., cardiovascular disease) of obesity.
As of 2014, four drugs (orlistat, phentermine/topiramate, liraglutide, and bupropion/naltrexone) were approved by the U.S. Food and Drug Administration (FDA) for long-term weight loss. Orlistat is available either by prescription (brand name Xenical) or over the counter (brand name Alli). Phentermine/topiramate (brand name Qsymia), liraglutide (brand name Saxenda), and bupropion/naltrexone (brand name Contrave) are available by prescription only. These weight-loss agents work by suppressing appetite or blocking pancreatic lipase.
Orlistat is a gastrointestinal and pancreatic lipase inhibitor that interferes with hydrolysis of dietary triglyceride and fatty acid absorption by the intestine [129]. It causes weight loss by blocking absorption of up to one-third of ingested fat. It is typically used with a reduced calorie diet with about 30% of calories from fat. Because absorption of fat-soluble vitamins can be affected, patients are advised to take a multivitamin daily. Several clinical studies have shown that when orlistat is combined with a low-calorie, low-fat diet, it increases weight loss compared with a placebo and low-calorie, low-fat diet. For example, in a randomized controlled trial conducted in Europe, patients using orlistat and eating a low-fat diet experienced a weight loss of 10.2% compared to 6.1% in the control group at one year [47]. In this study, total cholesterol, LDL, LDL/HDL ratio, and glucose showed a significant reduction. At year two, patients who continued with orlistat regained half as much weight as those patients who switched to placebo. In another randomized trial, patients using orlistat with a low-calorie diet experienced a loss of 8.5% of their initial body weight, compared with 5.4% in the placebo group [48]. Moreover, 35% of patients using orlistat lost at least 5% of body weight, compared with 21% in the placebo group; 28% lost 10% of body weight compared with 17% in control group. In a randomized controlled trial conducted in the United States, patients treated with orlistat lost an average of 15 lbs versus 8 lbs in the control group [49]. More patients in the experimental group lost 5% of initial weight than those in the control group, and 34% of patients using orlistat sustained the weight loss at two years versus 24% in the control group.
Orlistat is contraindicated in patients with chronic malabsorption syndrome or cholestasis, and it should be used with caution in patients taking cyclosporine. Side effects of orlistat include, but are not limited to, steatorrhea, incontinence, and diarrhea. Dietary supplementation with fat-soluble vitamins is recommended. Cases of acute kidney injury from oxalate crystal deposition have been reported in 2% of patients within one year of initiating orlistat [128]. Renal function should be monitored in patients receiving orlistat, particularly those at increased risk because of age or pre-existing renal dysfunction. Rarely, patients taking orlistat have developed severe liver injury, and this risk should be weighed against potential benefits [71].
In 2012, the FDA approved phentermine/topiramate, one of the first new weight-loss mediations in more than a decade [98]. Phentermine/topiramate (extended-release) combines an anorexiant and an anticonvulsant to improve short-term weight-loss outcomes in patients who have already attempted lifestyle changes (i.e., calorie-restricted diet and increased physical activity) [95]. Eligible patients will have a BMI ≥30 or a BMI ≥27 with a weight-related comorbidity [98]. In two randomized, placebo-controlled trials involving approximately 3,700 obese and overweight patients, phentermine/topiramate was found to be effective and safe if used correctly [98]. After one year, patients taking phentermine/topiramate experienced 6.7% (at the recommended dose) to 8.9% (at the highest dose) greater weight loss compared to those taking placebo. More than 60% of participants taking phentermine/topiramate recorded at least a 5% decrease in their body weight, compared to only 20% of the placebo group [98].
The recommended initial dose of phentermine/topiramate is 7.5 mg phentermine/46 mg topiramate extended-release once per day [98]. If weight reduction is <3% at 12 weeks, the dose may be titrated to a maximum of 15 mg/92 mg. The medication is contraindicated in persons with glaucoma, uncontrolled hypertension, or hyperthyroidism, and is not recommended for patients with a recent history of stroke or heart disease [98,128]. It is also teratogenic, with proven fetal defects with first trimester exposure. Therefore, all women of childbearing age should use effective contraception consistently while taking the drug and have documented proof of a negative pregnancy test prior to the initiation of treatment and every month thereafter [98].
In 2014, combination bupropion/naltrexone was approved as a treatment option for chronic weight management [99]. Studies show that these drugs are effective in improving the percentage of total body weight lost compared to placebo [84,99]. The dosage is gradually titrated up, starting with one tablet (naltrexone 8 mg/bupropion 90 mg) once daily in the morning for one week and increasing one daily tablet each week for four weeks. The maintenance dose is two tablets twice daily [71]. If 5% of initial body weight has not been lost after 12 weeks, the medication should be discontinued.
Any patient taking bupropion should be carefully monitored for suicidal ideation and behaviors [99]. This medication may also increase blood pressure and heart rate and is contraindicated in patients with hypertension. It also should be avoided in patients with opioid dependence, a history of seizures, or who are pregnant.
When pharmacotherapy is effective, weight loss should exceed 2 kg (4.4 lbs) during the first month and weight should decrease by about 5% of baseline within six months. Pharmacotherapy should be discontinued if weight loss is not achieved. In cases in which the therapeutic goal includes significant metabolic improvement in addition to weight loss (e.g., a patient with type 2 diabetes), failure to achieve a 5% decline in weight at three months warrants consideration of alternative pharmacotherapy or bariatric surgery [129]. When it is successful, pharmacotherapy with orlistat may be continued past one year; data is currently available to four years with orlistat [71]. Patients should keep in mind that weight loss typically stabilizes after six months of treatment, and weight gain can occur when pharmacologic therapy is discontinued.
In 2014, researchers conducted a systematic review to compare available FDA-approved drugs for short- and long-term weight loss using existing meta-analyses, systematic reviews, and randomized, placebo-controlled trials [114]. Combined with prescribed lifestyle changes, weight loss was noted at one year at approximately 3% for both orlistat and lorcaserin, and 9% for maximum-dose phentermine/topiramate compared with placebo [114]. Clinically meaningful weight loss (defined as ≥5% of initial weight in one year) was 37% to 47% for lorcaserin, 35% to 73% for orlistat, and 67% to 70% for maximum-dose phentermine/topiramate [114]. There were no short-term weight loss drugs that met the inclusion criteria for the analysis. Additional research, with the inclusion of the two more recently FDA-approved drugs (bupropion/naltrexone and liraglutide) is required to provide more information on the drug that provides the greatest efficacy [114].
Several drugs are approved for short-term use in obese patients. These include sympathomimetic agents such as benzphetamine, methamphetamine, phentermine, phendimetrazine, and diethylpropion [71,114]. Data on long-term safety have not been demonstrated. Given that weight loss therapy is focused on long-term success, use of these drugs is rarely recommended. Leptin resistance may be a contributing factor to obesity in some cases, and leptin is being explored as a possible treatment.
The cannabinoid receptor antagonist rimonabant, which acts as an appetite suppressant, has shown promise for weight loss. It is currently available in Europe. However, the FDA declined to approve this drug for use in the United States, citing concerns about the risk-benefit profile and the need for more data. In the future, rimonabant or similar drugs may become available in the United States.
Two additional drugs, silbutramine in 2010 and lorcaserin in 2012, initially received FDA approval for weight management but were later withdrawn because of safety issues. Randomized controlled trials supported the efficacy of sibutramine for short-term weight loss; however, there was some concern regarding the cardiovascular risk profile associated with the medication [50,51,52]. Postmarketing data indicated that patients with existing cardiovascular disease on long-term sibutramine therapy had an increased risk of nonfatal myocardial infarction and stroke [53]. As a result, the manufacturer (Abbott Laboratories) responded to an FDA request by voluntarily removing the agent from the U.S. market in 2010 [72]. Lorcaserin was voluntarily withdrawn from the market by the manufacturer in 2020 due to results from safety clinical trials showing an increased occurrence of cancer [95]. Other previously available drugs included dexfenfluramine and fenfluramine. Both have been withdrawn from the market due to either increased risk of pulmonary arterial hypertension or valvular heart disease.
Glaucon-like peptide-1 (GLP-1) is an incretin metabolic hormone secreted in the intestinal tract, pancreas, and central nervous system (predominantly the brainstem). GLP-1 has several physiologic effects important for energy balance, regulation of glucose, and control of appetite and food intake [65]. Eating food triggers the release of GLP-1, which in turn inhibits glucagon secretion, promotes insulin production, and prompts feelings of fullness (satiety) via central effects on neural pathways [66]. Thus, GLP-1 has an important role in facilitating and maintaining healthy body weight. GLP-1 exerts its action through a single GLP-1 receptor that is widely expressed in human tissues. In the past decade, analogs of the GLP-1 receptor (GLP-1 agonists) have been developed that mimic the action and prolong the effects of GLP-1. Compared with native GLP-1, which has a short half-life (1.5 to 2 minutes), GLP-1 agonists have a longer half-life (hours to days), permitting augmentation of GLP-1 physiologic effects and engendering intense interest in GLP-1 agonists as therapeutic agents for long-term weight control and prevention of obesity-related comorbidities.
Studies in human volunteers have shown that activation of GLP-1 receptors, whether by endogenous GLP-1 or GLP-1 agonists, has several important effects conducive to weight management in obese and overweight persons. GlP-1 infusion in the fasting state prompted a sensation of fullness (satiety) and diminished the perception of hunger, findings which correlated with reduced brain activation in the amygdala, caudate, and cortical brain centers [65]. When eating a meal, administration of a GLP-1 has been shown to reduce food intake and attenuate brain activation to pictures of food in obese persons and those with heightened sensitivity to food cues [65]. A randomized, placebo-controlled trial found that compared with placebo, a GLP-1 agonist (liraglutide) enhanced satiation (maximum tolerated intragastric volume) and delayed gastric emptying of solids by 70 minutes vs. 4 minutes at five weeks [67]. Post-hoc analysis showed that delayed gastric emptying of solids at 5 weeks correlated with significantly greater weight loss in the liraglutide group than in the placebo group at 5 weeks and 16 weeks.
As of January 2024, two GLP-1 agonists, liraglutide and semaglutide, have received FDA approval for chronic weight management in obese and overweight patients with or without diabetes, A third drug, tirzepatide, which is a dual-action combination agent (GLP-1 agonist with a glucose-dependent insulinotropic polypeptide) has also received FDA approval. Tirzepatide exhibits enhanced activity in regulating glucose-dependent insulin release and may have an advantage managing patients with type 2 diabetes and obesity. When using any one of these drugs for weight management, gradual dosage escalation over 16 to 20 weeks is necessary to reduce likelihood of adverse effects.
Liraglutide
In 2014, the GLP-1 receptor agonist liraglutide was approved by the FDA for chronic weight management. Traditionally used to treat diabetes, liraglutide also aids in appetite suppression and weight loss [109]. The dosage of liraglutide used for weight management (3 mg) differs from the dose used in diabetes medication regimens (1.8 mg), and the safety and efficacy of this higher dose for the treatment of diabetes is uncertain [109]. Liraglutide is administered subcutaneously, and when used for management of obesity, it should be initiated at 0.6 mg once daily and escalated weekly by 0.6 mg up to 3 mg [128]. Common side effects are nausea (25%), vomiting (12%), diarrhea (11.6%), constipation (11%), and dyspepsia (6.4%). A meta-analysis found that liraglutide has the highest probability of discontinuation due to side effects (13% of patients) among all FDA-approved medications for obesity [128]. This medication is contraindicated in those with a personal or family history of thyroid cancer.
Patients with type 2 diabetes and high cardiovascular risk randomized to treatment with liraglutide had a 22% decrease in cardiovascular mortality and 15% decrease in all-cause mortality compared with placebo after 3.8 years [128]. Among adolescents with obesity, liraglutide plus lifestyle therapy was two times more effective than lifestyle therapy alone (43.3% vs. 18.7%) in reducing BMI by 5%, and three times more effective (26% vs. 8%) in reducing BMI by 10% [130].
Semaglutide
In 2021, the FDA approved semaglutide injection for chronic weight management in adults with obesity (BMI ≥30), or overweight (BMI ≥27) with at least one additional weight-related comorbidities (e.g., hypertension, type 2 diabetes, hyperlipidemia) [133]. Semaglutide is a GLP-1 receptor agonist intended for use in combination with lifestyle changes. For weight management, the dosage of semaglutide is 2.4 mg subcutaneously administered weekly [133]. In one study involving 1,961 obese or overweight adults who did not have diabetes, once weekly semaglutide was associated with an average weight loss of 15.3 kg after 68 weeks, compared with 2.6 in the placebo group [134]. More participants in the semaglutide group than in the placebo group achieved weight reductions of 10% or more (69.1% vs. 12%) and 15% or more (50.5% vs. 4.9%) at week 68. Mild-to-moderate nausea and diarrhea were the most common adverse events with semaglutide and subsided over time [134]. Compared with placebo, weight loss with semaglutide was accompanied by greater improvements in cardiometabolic risk factors, including reductions in waist circumference, blood pressure, glycated hemoglobin levels, and lipid levels.
In a separate phase 3 clinical trial among adolescents (12 to <18 years of age) with obesity (BMI in the 95th percentile or higher), treatment with weekly semaglutide plus lifestyle intervention resulted in a greater reduction in BMI than lifestyle intervention alone [93]. The mean change in BMI at week 68 was –16.1% with semaglutide and 0.6% with placebo. A total of 95 of 131 participants (73%) in the semaglutide group had weight loss of 5% or more, compared with 11 of 62 (18%) in the placebo group. Among participants in the semaglutide group, a loss of body weight of at least 10% occurred in 62% and of least 15% in 53%, compared with 8% and 5%, respectively, among those in the placebo group [93].
Results of a multicenter randomized, placebo-controlled trial has demonstrated that treatment with semaglutide diminishes excess cardiovascular risk associated with obesity and overweight in patients who have no history of diabetes. The study, which enrolled 17,610 participants with a BMI of 27 or greater and preexisting cardiovascular disease, found that weekly subcutaneous simaglutide at a dose of 2.4 mg for a mean duration of 33 months was associated with a 20% reduction in the incidence of a composite of death from cardiovascular causes, nonfatal myocardial infarction, and nonfatal stroke, compared with placebo [94].
Evidence suggests semaglutide may also be effective in alleviating symptoms and signs of heart failure with preserved ejection fraction associated with obesity. In a randomized, placebo-controlled trial involving obese patients with this syndrome, once weekly semaglutide achieved larger reductions in heart failure-related symptoms and physical limitations, increased functional capacity, and more weight loss than placebo (–13.3% vs. –2.6%) at 52 weeks [106]. The mean percentage change in C-reactive protein (surrogate for ambient inflammation) was –43.5% with semaglutide and –7.3% with placebo. The authors note that the magnitude of improvement in physical function observed in the semaglutide group, as measured by the six-minute walk distance, was greater than or equal to results reported in studies designed to investigate outcomes of exercise training in in patients with heart failure [106].
Tirzepatide
In 2022, the FDA approved weekly tirzepatide injection for the treatment of type 2 diabetes [135]. In studies of the drug's efficacy in lowering blood glucose levels, patients were also found to experience significant weight loss; in one clinical trial, the average weight loss with tirzepatide was 15 pounds more than placebo when neither were used with insulin and 23 pounds more than placebo when both were used with insulin [135]. In a study of 2,539 obese adults without diabetes, after 72 weeks of treatment, the mean percentage change in weight 72 was −15.0% for those receiving 5-mg tirzepatide, −19.5% for those receiving 10-mg tirzepatide, and −20.9% for those receiving 15-mg tirzepatide; the percent change among those who received placebo was −3.1% [136]. Additional trials are underway to assess the potential role of tirzepatide in the treatment of obesity.
In November 2023, the FDA approved tirzepatide injection for chronic weight management in adults with obesity (BMI ≥30) or overweight (BMI ≥27) with at least one weight-related condition (e.g., high blood pressure, type 2 diabetes, hyperlipidemia) [107]. Effectiveness of tirzepatide for weight management was established in two randomized, placebo-controlled trials conducted for 72 weeks' duration, each demonstrating significant reduction in body weight compared with placebo. This approved tirzepatide formulation (Zepbound) is administered weekly; the dosage must be increased gradually over four to 20 weeks to achieve the target dosage of 5 mg, 10 mg, or 15 mg once weekly [107]. The maximum dosage is 15 mg once weekly.
Practical Considerations for GLP-1 Agonist Therapy
Clinical trial experience has shown that mild-to-moderate adverse effects occur commonly with GLP-1 agents but resolve in time and can be minimized by gradual dosage escalation over 16 to 20 weeks' time. The most common side effects are gastrointestinal, including nausea, vomiting, diarrhea, and abdominal discomfort. Less common but more serious adverse effects observed in large clinical trials include symptomatic gall bladder/biliary tract disease (2.5%) and pancreatitis (0.2%) [66,134]. GLP-1 agonists are known to cause mild inhibition of gall bladder emptying and biliary tract peristalsis. To ensure compliance and maximum therapeutic success, treatment of obesity with GLP-1 agonists should always be initiated slowly with gradual dosage escalation and careful follow-up, including patient education and reassurance as to anticipated (and likely self-limited) adverse effects. Other suggestions for a successful treatment strategy include a multidisciplinary approach with telephone surveillance; avoiding high-fat foods and utilizing frequent small meals; a one-week dose pause when adverse effects do arise [108].
Surgery offers the most effective intervention for reducing the long-term complications of obesity and related metabolic disorders such as diabetes [17,131]. High morbidity and mortality rates are associated with severe obesity (BMI >40) and with a BMI of 35 to 39 in the presence of a coexisting condition. With refinement in surgical technique and growing evidence of safety and efficacy, bariatric surgery has become increasingly common over the past decade. In 1998, there were 13,386 procedures; by 2004, nearly 136,000 bariatric surgeries were performed [55,85]. Since then, the number has continually increased, with approximately 262,893 surgeries performed in 2021 [104]. Only 1% of the extremely obese population undergoes bariatric surgeries each year [85,86,87]. In 2008, 90.2% of bariatric surgeries were performed laparoscopically, compared with 20.1% in 2003. Surgical procedures for overweight and obese patients include:
Gastric bypass
Gastric banding
Vertical banded gastroplasty
Sleeve gastrectomy
Intestinal bypass
The American Society of Metabolic and Bariatric Surgery (ASMBS) and International Federation for the Surgery of Obesity and Metabolic Disorders assert that metabolic and bariatric surgery is recommended for individuals with a BMI >35, regardless of presence, absence, or severity of comorbidities.
(https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9834364 Last Accessed: January 18, 2024)Level of Evidence: Expert Opinion/Consensus Statement
The American Society for Metabolic and Bariatric Surgery (ASMBS) and the Society of American Gastrointestinal Endoscopic Surgeons have reaffirmed the 1991 National Institutes of Health guideline, which states that surgery is indicated for adult patients with a BMI greater than 40 or greater than 35 with significant comorbid conditions and who can demonstrate that dietary attempts at weight loss have failed [56,57]. In 2022, guidelines from the International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO) and ASMBS were released establishing the criteria for candidates for bariatric surgery as BMI ≥35, regardless of presence, absence, or severity of obesity-related complication, or BMI ≥30 in patients with type 2 diabetes [96]. Further, surgery should also be considered in patients with BMI 30–35 who do not achieve substantial or durable weight loss or obesity-related complication improvement nonsurgically. In 2019, the AACE/TOS/ASMBS/Obesity Medicine Association (OMA)/American Society of Anesthesiologists (AASA) guidelines further added a recommendation that the BMI requirement for bariatric surgery should be adjusted for ethnicity (e.g., 18.5 to 22.9 is normal range, 23 to 24.9 is overweight, and ≥25 is obesity for Asian patients) [97]. The 2022 ASMBS guideline recommends BMI thresholds be adjusted in Asian populations, and those with BMI >27.5 should be offered surgery ]96].
In 2016, 45 professional societies, including the American Diabetes Association, issued a joint statement that metabolic surgery should be considered for patients with type 2 diabetes and a BMI 30.0–34.9 if hyperglycemia is inadequately controlled despite optimal treatment with either oral or injectable medications [98].
Bariatric surgery for patients older than 60 years of age has typically not been recommended. Patients should be thoroughly screened for a willingness to make lifestyle changes, as well as for any psychologic disorders that would impair a successful postoperative course. Surgical treatment is not a cosmetic procedure. It does not involve the removal of adipose tissue by suction or excisions; rather, it involves reducing the size of the stomach, with or without a degree of malabsorption.
In addition to those patients identified in the 1991 guideline, the Society of American Gastrointestinal Endoscopic Surgeons indicates that other well-selected patients may benefit from laparoscopic bariatric surgery [57]:
Individuals with BMI 30–35
Patients older than 60 years of age
Select adolescents
Adolescent bariatric surgery (in patients younger than 18 years of age) has been proven effective but should be performed in a specialty center. Patient selection criteria should be the same as used for adult bariatric surgery.
Research supports the effectiveness of bariatric surgery for weight loss, and although more outcome data have been made available since the 2000s, additional studies are required to prove long-term outcomes [91,115]. In the Swedish Obese Subjects (SOS) study, a large, prospective, controlled trial of bariatric surgery (fixed or variable banding, vertical banded gastroplasty, or gastric bypass), average weight loss in surgical patients was 16% at 10 years compared to a 1.6% weight gain in controls [58]. A 2005 Cochrane Review, which included earlier SOS results as well as multiple other studies, noted that evidence was limited (largely due to study design), but that surgery appeared to be more effective than conventional treatment [59]. A meta-analysis published in 2004 in JAMA concluded that mean excess weight loss was 61.2% for bariatric surgery patients, with some variation among types of surgery [60]. One long-term systematic review used MEDLINE and Cochrane databases to analyze research from 1946 to 2014 and found that there is still insufficient long-term patient follow up needed to minimize biased results. In this review, it was found that found that gastric bypass has better outcomes than gastric band procedures; however, there was insufficient evidence regarding other types of bariatric procedures, including gastric sleeve [115].
It also appears that weight loss following bariatric surgery may be more sustainable than weight loss by conventional means. While weight regain often occurs within a few months to years after behavioral or pharmacologic treatment, studies show that weight loss can be sustained for many years after surgery [55]. A large, single-center follow-up study of laparoscopic adjustable gastric banding patients showed the band was intact in 78% of patients beyond the 10-year follow-up, with a mean excess weight loss of 47% [103]. At the 16-year mark, patients had an excess weight loss of 62%. The authors of the study reviewed other literature and noted a similar substantial long-term weight loss with other bariatric surgeries as well.
Although bariatric surgery is not without risk, there is evidence that it can reduce overall morbidity and mortality in obese patients. In a cohort study comparing 1,035 bariatric surgery patients with 5,746 age- and gender-matched controls, the surgery patients had significant reductions in the risk of cardiovascular disease, cancer, endocrine disorders, infections, and psychiatric disorders. The relative risk of death was 89% lower in the surgery group [61]. Another study compared 7925 gastric bypass subjects with community-based controls. Mortality was lower by 40% among the surgery patients. Although deaths from causes other than disease were higher in the surgery patients, deaths from diabetes, cardiovascular disease, and cancer were all substantially reduced [62]. The SOS study, the only large, well-controlled prospective trial of bariatric surgery, found the unadjusted overall mortality was reduced by 31.6% in the surgery group at 10 years [63].
Multiple studies of comorbid conditions that are common in obesity have shown improvement following bariatric surgery. A meta-analysis of bariatric surgery studies showed strong improvements in diabetes, hypertension, hyperlipidemia, and sleep apnea [60]. According to results from the SOS study, some of the improvements in morbidity may decrease over time; however, longer observation and additional studies are needed to confirm long-term effects [58].
These procedures combine creation of small stomach pouches to restrict food intake and construction of bypasses of the duodenum and other segments of the small intestine to cause malabsorption. In the past, the most common gastric bypass operation was Roux-en-Y gastric bypass (RYGB), with biliopancreatic diversion performed less frequently [104]. According to one report, in 2003–2004 more than 90% of the weight-loss surgeries performed in the United States involved the Roux-en-Y technique, even though this surgery required longer time in surgery, longer hospital stays, and a higher likelihood of requiring intensive care [63]. However, the advent of newer and less invasive techniques has led to these surgeries falling out of favor. In 2021, the ASMBS estimated that only 21.5% of bariatric surgeries involved RYGB and 2.1% were biliopancreatic diversion [104]. Today, sleeve gastrectomy is the most commonly performed procedure (58.1%) [104].
In the SOS study, the gastric bypass group lost the most weight, compared to banding and vertical banded gastroplasty; they were also more likely to have lost more than 5% of baseline body weight [58]. A meta-analysis of multiple studies concluded that weight loss was about 61.6% with gastric bypass and 70.1% with biliopancreatic diversion, vs. 47.5% for gastric banding. However, these procedures also carry a higher risk of nutritional deficiency.
Roux-en-Y Gastric Bypass (RYGB)
With gastric sleeve procedures becoming more common, only 21.5% of bariatric surgeries performed in 2021 were RYGB procedures [104]. In this procedure, a small stomach pouch, approximately 25–30 mL in size, is created by either stapling or vertical banding. This causes restriction in food intake, such that patients can only eat several bites as a meal. Next, a Y-shaped section of the small intestine is attached to the pouch to allow food to bypass the duodenum as well as the first portion of the jejunum. This causes reduced calorie and nutrient absorption, resulting in weight loss. Gastric bypass is usually done laparoscopically.
With this procedure, severe nutritional deficiencies can develop. For instance, patients are at risk to develop iron deficiency due to lack of food contact with gastric acid and consequent diminished conversion of iron. In addition, vitamin B12 deficiency may occur because food is not coming into contact with gastric intrinsic factor. Vitamin D and calcium absorption may be reduced because the duodenum and proximal jejunum, which are the sites of calcium absorption, are bypassed. Lifelong supplements of multivitamins, B12, iron, and calcium are mandatory following this procedure.
Biliopancreatic Diversion (BPD) and Biliopancreatic Diversion with Duodenal Switch (BPD/DS)
In the BPD and BPD/DS operations, portions of the stomach (approximately two-thirds) are removed. The small pouch that remains is connected directly to the final segment of the small intestine, completely bypassing both the duodenum and jejunum. Thus, the time that food mixes with digestive fluids is fairly brief.
In biliopancreatic diversion with duodenal switch the pyloric valve is kept intact, a portion of the duodenum is left in the digestive loop, and the final segment of the small intestine is connected after the duodenum. Additionally, the upper end of the bypassed segment of the small intestine is attached to the pancreas and is joined at the final, common segment. The gallbladder may or may not be removed.
Restrictive procedures reduce the size of the stomach without interfering with absorption of food. Food intake is restricted by creating a small pouch at the top of the stomach where the food enters from the esophagus. The pouch initially holds about 1 ounce of food and can expand to 2 to 3 ounces over time. The pouch's lower outlet usually has a diameter of about ¼ inch. The small outlet delays the emptying of food from the pouch and causes a feeling of fullness. It does not otherwise alter the digestive tract. Restriction operations are intended to reduce the amount of food a patient can comfortably eat, thus reducing total caloric intake. The two most common restriction operations are gastric banding and vertical banded gastroplasty.
Laparoscopic Gastric Banding (LGB)
In this procedure, a band is placed around the stomach near its upper end, creating a small pouch and a narrow passage into the larger remainder of the stomach. An inflatable, adjustable ring controls the flow of food from the smaller pouch to the rest of the digestive tract. The patient will feel comfortably full with a small amount of food. Because of the slower emptying, the patient continues to feel full for several hours, thereby reducing the urge to eat between meals.
Although excess weight loss with this procedure is not as rapid as with other procedures (e.g., RYGB), long-term weight loss may be comparable for some patients [90,91]. One study found that weight loss percentages for RYGB and LGB were 35% and 19% after three months; 49% and 25% after six months; 64% and 36% after one year; and 60% and 57% after three years [90]. However, other studies report that about half of LGB procedures result in inadequate weight loss [92]. A 2008 systematic review noted that complication and short-term morbidity rates of LGB are lower than those of laparoscopic RYGB; however, reoperation rates with LGB are higher [91]. This review noted that the highest quality study showed an excess weight loss percentage at one year of 48% for LGB, compared with 76% for RYGB.
It appears that LGB has quickly fallen out of favor. LGB accounted for 35.4% of bariatric procedures in 2011 but only 0.4% in 2021 [104].
Vertical Banded Gastroplasty (VBG)
In this procedure, both a band and staples are used to create a small pouch in the upper stomach with a narrow outlet reinforced by a mesh band to prevent stretching. After the procedure, the person usually can eat only a half to a whole cup of food without discomfort or nausea. Food must be well chewed. VBG, formerly one of the most common bariatric surgeries, is used less often now due to unsatisfactory weight loss results [55]. Complications from the restriction can include vomiting, gastroesophageal reflux, and erosion of the band into the gastric tissue.
Neither of these procedures involves any anastomosis of the stomach or intestine, nor is there repositioning of the stomach or intestines. Intake becomes a function of a patient's ability to chew thoroughly and eat slowly. Failure to do so can result in repeated vomiting and isolated cases of nutritional deficiency.
Laparoscopic Sleeve Gastrectomy (LSG)
Similar to the first step of BPD, laparoscopic sleeve gastrectomy (LSG) involves subtotal gastric resection, leaving a small, tubular stomach [88]. Because the fundus of the stomach contains the cells that produce ghrelin (a hormone involved in regulation of food intake), removal of the fundus may contribute to weight loss beyond simple restriction. LSG is generally done in select obese and super-obese (BMI greater than 50) patients and followed, once weight is somewhat reduced, by completion of a RYGB or either of the BPD surgeries. Advantages of this approach include simplicity, low complication rates, no nutritional deficiencies, and no "dumping syndrome" [88].
A 2009 study of 135 patients who underwent the procedure (mean BMI: 48.8; range: 37–72) found that the average excess weight loss at one year was 49.4% [89]. Complication rates were low, and none of the patients required conversion to laparotomy.
A 2010 review of 100 LSG patients (BMI greater than 40 or greater than 35 with severe comorbidity) found that the average excess weight loss was 49.1% at six months [88]. There was also significant resolution of diabetes (46%), hypertension (38%), and hyperlipidemia (19%). The authors of the study recommend LSG as a single-step procedure, with no revision to RYGB or BPD, and LSG over gastric banding due to equivalent weight reduction and better tolerance.
Bariatric surgery does have complications. Approximately 10% to 20% of all patients who have weight-loss surgery require follow-up operations. Gastric bypass operations may cause "dumping syndrome," whereby stomach contents move too rapidly through the small intestine. Typically, this is caused by the high osmolarity of simple carbohydrates in the intestine. The higher concentration causes fluids to shift towards the higher osmolarity. This results in additional fluid in the bowel, which causes it to be stretched, with subsequent pain and nausea. Activation of hormonal and nerve responses causes increased heart rate. There may be vomiting and diarrhea. A short time later, there typically is a glucose spike, as the small bowel absorbs sugar. The pancreas responds by secreting insulin, which then causes hypoglycemia, causing weakness and light-headedness. Dumping syndrome should be monitored carefully.
Abdominal hernias can also occur, requiring follow-up surgery. More than one-third of obese patients who have gastric surgery develop gallstones. Post-operative complications may include deep vein thrombosis, pulmonary emboli, bleeding, band migration, and infection. Possible later complications include breakdown of the staple line or band erosion, causing internal infections.
Depending on the type of procedure, nearly 30% of patients who have weight-loss surgery can develop nutritional deficiencies such as anemia, osteoporosis, and metabolic bone disease. Therefore, it is important that patients take supplemental vitamins and minerals.
Because bariatric surgical procedures are still evolving, true surgical mortality rates are uncertain. The overall risk of death from gastric bypass appears to be less than 0.2% at 30 days and varies by the type of procedure [105]. Older data, gathered between 1987 and 2001, suggested a 30-day mortality rate as high as 1.9%, but outcomes have improved as surgeons gained experience and lower-risk patients sought treatment [55]. The increase in laparoscopic procedures has contributed to a lower risk of death. It is estimated that the 30-day mortality rate is 0.14% for laparoscopic gastric bypass, 0.08% for laparoscopic sleeve gastrectomy, and 0.03% for laparoscopic gastric banding [105].
The appropriate surgery depends on a number of factors, including the skill of the surgeon and patient preference. Typically, restriction operations create slower and steadier weight loss than the bypass operations, which often show rapid weight loss in the first few months, stabilizing a year after surgery. With restriction operations, weight loss is typically 1 to 2 pounds per week, continuing on average for two years. However, restriction operations have higher potential for nutritional deficiency.
Bariatric surgery will not work for all patients. Between 10% and 50% of surgical subjects will not succeed with long-term weight loss [55,92]. Ongoing follow-up is an essential part of treatment, to watch for complications and encourage ongoing weight loss efforts.
Intragastric balloon systems, brand names Orbera and the ReShape Integrated Balloon System, were approved by the FDA in 2015. These systems are intended as a minimally invasive, short-term treatment, involving placement in the stomach of an inflatable, free-floating balloon. They are intended to be used in conjunction with diet and exercise. Both Orbera and ReShape are placed into the stomach through the mouth with the patient under mild sedation, using a minimally invasive endoscopic procedure. These balloons are then filled with 400–700 cc of saline (ReShape also adds methylene blue dye) to restrict the amount of space in the stomach. These balloons may be placed for up to six months. A third balloon system, brand name Obalon, was approved by the FDA in 2016 and consists of up to three balloons in a capsule that is attached to a thin inflation catheter. The balloons are swallowed and then inflated with air to reduce amount of free space in the stomach [117].
Intragastric balloon systems may have indications for individuals with BMIs between 30 and 40 and for morbidly obese patients who need to lose weight before bariatric surgery. A 2007 Cochrane Review suggests that intragastric balloon treatment may not provide benefits over conventional therapy. However, evidence was limited and different trials used different techniques and clinical considerations [64].
Little information is available regarding the effectiveness and long-term indications of balloon systems. In clinical trials for Orbera, patients lost an average of 21.8 lbs (10.2% total body weight) after six months, compared with 7 lbs in the same period in a group that received behavior modification. In addition, three months after placement, patients maintained an average weight loss of 19.4 lbs [118].
In February 2017, the FDA issued a letter to healthcare providers warning that there have been incidences of spontaneous overinflation of the two brands of liquid-filled balloons (Orbera and ReShape), causing abdominal pain, difficulty breathing, and vomiting [117]. A risk of acute pancreatitis caused by compression of gastrointestinal structures was also noted. Additionally, in August 2017, the FDA issued a letter to healthcare providers warning of adverse events associated with the saline-inflated versions (Orbera and ReShape). It was noted that five unanticipated deaths had occurred—one patient with ReShape and four with Orbera. A follow up letter was issued in April 2020, indicating a total of 18 deaths reported worldwide; of these, 8 were in the United States (5 with Orbera and 3 with ReShape) [132]. At the time of publication of the letter, there was no known root cause, although all patients died within hours to six months of placement [117]. Further investigation of the safety and effectiveness of these balloon devices is required.
Gastric electrical stimulation is a technique involving an implanted device similar to a cardiac pacemaker. In 2015, the FDA approved the Maestro Rechargeable System for the treatment of obesity in patients 18 years or older with a BMI of 40 to 45, or 35 to 39.9 with one or more obesity-related health condition. In addition, the patient must have tried to lose weight with diet and exercise in a supervised program within the past five years.
Controllable from outside the body, the gastric stimulator is intended to reduce caloric intake [55]. The Maestro device is implanted into the abdomen and entails an electronic pulse generator that sends impulses to the vagus nerve. The wire leads and electrodes then directly stimulate the vagus nerve to control appetite. A study of those using the Maestro device showed that the active group lost 8.5% more weight than the placebo group. In addition, 52.5% of the active electronic device group lost at least 20% of excess weight and 38.3% lost at least 25% of their starting weight [119]. Studies are ongoing, and as of 2018 there is no reliable data on the long-term efficacy of gastric electrical stimulation.
As a result of the evolving racial and immigration demographics in the United States, interaction with patients for whom English is not a native language is inevitable. Because patient education is such a vital aspect of the prevention and treatment of overweight and obesity and related conditions, it is each practitioners' responsibility to ensure that information and instructions are explained in such a way that allows for patient understanding. When there is an obvious disconnect in the communication process between the practitioner and patient due to the patient's lack of proficiency in the English language, an interpreter is required.
In this multicultural landscape, interpreters are a valuable resource to help bridge the communication and cultural gap between clients/patients and practitioners. Interpreters are more than passive agents who translate and transmit information back and forth from party to party. When they are enlisted and treated as part of the interdisciplinary clinical team, they serve as cultural brokers, who ultimately enhance the clinical encounter.
The number of overweight and obese people has reached epidemic proportions. Estimates show that 78% of the adult population is either overweight, obese, or extremely obese. This represents a substantial increase from the last few decades. Ample scientific evidence exists that demonstrates an increasing body mass index corresponds to increasing morbidity and mortality. Numerous treatments for obesity are available. The cornerstone of any treatment regimen is behavioral modification, focusing on diet changes and exercise regimens. Additional therapies include drugs and surgery. To improve care for overweight and obese patients, physicians and other providers need to have a thorough understanding of obesity and its treatment and to understand the importance of addressing the topic with patients. In addition, they must recognize that recidivism and failure are quite high, and that successful treatment requires a concerted and sustained effort. As of 2024. GLP-I agonists are a promising new class of therapeutic agents approved for long-term weight management in obese and overweight patients with and without type 2 diabetes. The degree of weight reduction and demonstrated benefits with respect to reducing comorbidities and complications from obesity rival that achieved with the best surgical therapies.
| CDC Resources and Publications for Overweight and Obesity |
| https://www.cdc.gov/obesity/resources/index.html |
| Managing Overweight and Obesity in Adults: Systematic Evidence Review from the Obesity Expert Panel |
| https://www.nhlbi.nih.gov/health-topics/managing-overweight-obesity-in-adults |
| Dietary Guidelines for Americans |
| https://health.gov/our-work/nutrition-physical-activity/dietary-guidelines |
| Physical Activity Guidelines for Americans, 2nd Edition |
| https://health.gov/sites/default/files/2019-09/Physical_Activity_Guidelines_2nd_edition.pdf |
| National Institute on Aging, Exercise and Physical Activity |
| https://www.nia.nih.gov/health/exercise-and-physical-activity |
| AHA Diet and Lifestyle Recommendations |
| https://www.heart.org/en/healthy-living/healthy-eating/eat-smart/nutrition-basics/aha-diet-and-lifestyle-recommendations |
| Institute of Medicine (IOM) Dietary Reference Intakes for Energy, Carbohydrates, Fiber, Fat, Protein, and Amino Acids |
| https://nap.nationalacademies.org/read/10490/chapter/1 |
| U.S. Preventive Services Task Force Guide to Clinical Preventive Services |
| https://www.ahrq.gov/professionals/clinicians-providers/guidelines-recommendations/guide/index.html |
1. Hales CM, Carroll MD, Fryar CD, Ogden CL. Prevalence of obesity and severe obesity among adults: United States, 2017–2018. NCHS Data Brief. 2020;360:1-7.
2. Centers for Disease Control and Prevention. Data Trends and Maps: Physical Activity—Behavior. Available at https://nccd.cdc.gov/dnpao_dtm/rdPage.aspx?rdReport=DNPAO_DTM.ExploreByTopic&islClass=PA&islTopic=PA1&go=GO. Last accessed January 13, 2024.
3. Lee-Kwan SH, Moore LV, Blanck HM, et al. Disparities in state-specific adult fruit and vegetable consumption—United States, 2015. MMWR. 2017;66:1241-1247.
4. Moore, LV, Thompson FE, Demissie Z. Percentage of youth meeting federal fruit and vegetable intake recommendations, Youth Risk Behavior Surveillance System, United States and 33 states, 2013. Journal of the Academy of Nutrition and Dietetics. 2017;117(4):545-553.
5. Finkelstein EA, Trogdon JG, Cohen JW, Dietz W. Annual medical spending attributable to obesity: payer-and service-specific estimates. Health Aff (Millwood). 2009;28(5):w822-w831.
6. U.S. Department of Health and Human Services, Public Health Service, Office of the Surgeon General. The Surgeon General's Call to Action to Prevent and Decrease Overweight and Obesity. Available at https://www.ncbi.nlm.nih.gov/books/NBK44206. Last accessed January 16, 2024.
7. Allison DB, Fontaine KR, Manson JE, Stevens J, VanItallie TB. Annual deaths attributable to obesity in the United States. JAMA. 1999;282(16):1530-1538.
8. Flegal KM, Graubard BI, Williamson DF, Gail MH. Excess deaths associated with underweight, overweight, and obesity. JAMA. 2005;293(15):1861-1867.
9. Bray B. Definitions and proposed current classification of obesity. In: Bray B, Bouchard C (eds). Handbook of Obesity. 4th ed. New York, NY: CRC Press; 2014.
10. National Task Force on the Prevention and Treatment of Obesity. Overweight, obesity, and health risk. Arch Intern Med. 2000;160(7):898-904.
11. National Heart, Lung, and Blood Institute. Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults: The Evidence Report. Available at https://www.ncbi.nlm.nih.gov/books/NBK2003. Last accessed January 16, 2024.
12. Adams KF, Schatzkin A, Harris TB, et al. Overweight, obesity, and mortality in a large prospective cohort of persons 50 to 71 years old. N Engl J Med. 2006;355(8):763-778.
13. U.S. Department of Defense. Directive Number 1308.1: Physical Fitness and Body Fat Program. Available at https://www.esd.whs.mil/portals/54/documents/dd/issuances/dodi/130803p.pdf. Last accessed January 16, 2024.
14. Centers for Disease Control and Prevention. Childhood Obesity Facts. Available at: https://www.cdc.gov/obesity/data/childhood.html. Last accessed January 13, 2024.
15. Redfield MM, Borlaug BA. Heart failure with preserved ejection fraction: a review. JAMA. 2023;329:827-838.
16. Centers for Disease Control and Prevention. Adult Obesity Facts. Available at https://www.cdc.gov/obesity/data/adult.html. Last accessed January 13, 2024.
18. Brown P, Bentley-Condit V. Culture, evolution and obesity. In: Bray GA, Bouchard C. Handbook of Obesity. 4th ed. New York, NY: CRC Press; 2014.
19. Zhang Y, Proenca R, Maffei M, et al. Positional cloning of the mouse obese gene and its human homologue. Nature. 1994;372(6505):425-432.
20. Coleman DL. Obese and diabetes: two mutant genes causing diabetes-obesity syndromes in mice. Diabetologia. 1978;14(3):141-148.
21. Perusse L, Chagnon YC, Weisnagel J, Bouchard C. The human obesity gene map: the 1998 update. Obesity Research. 1999;7(1):111-129.
22. Barlow SE, Dietz WH. Obesity evaluation and treatment: expert committee recommendations. Pediatrics. 1998;102:1-11.
24. National Cancer Institute. Cancer Prevention Overview. Available at https://www.cancer.gov/about-cancer/causes-prevention/hp-prevention-overview-pdq. Last accessed January 16, 2024.
25. Huang Z, Hankinson SE, Colditz GA, et al. Dual effects of weight and weight gain on breast cancer risk. JAMA. 1997;278(17):1407-1411.
26. Hinderliter A, Sherwood A, Gullette EC, et al. Reduction of left ventricular hypertrophy after exercise and weight loss in overweight patients with mild hypertension. Arch Intern Med. 2002;162:1333-1339.
27. U.S. Department of Health, Education, and Welfare. Report of the United States National Commission on Diabetes to the Congress of the United States. Pub. 76-1021. Washington, DC: U.S. Department of Health, Education, and Welfare; 1975.
28. Michaud DS, Giovannucci E, Willett W, et al. Physical activity, obesity, height, and the risk of pancreatic cancer. JAMA. 2001;286(8):921-929.
30. Olson C, Schumaker H, Yawn B. Overweight women delay medical care. Arch of Fam Med. 1994;3(10):888-892.
31. Foster G., Wadden T, Phelan S, Sarwer D, Sanderson RS. Obese patients' perceptions of treatment outcomes and the factors that influence them. Arch Intern Med. 2001;161:2133-2139.
32. Blackwell DL, Lucas JW, Clarke TC. Summary health statistics for U.S. adults: National Health Interview Survey, 2012. Vital Health Stat. 2014;10(260).
33. Foster GD, Wyatt HR, Hill DO, et al. A randomized trial of a low-carbohydrate diet for obesity. N Engl J Med. 2003;348(21):2082-2090.
34. Dansinger ML, Gleason JA, Griffith JL, Selker HP, Schaefer EJ. Comparison of the Atkins, Ornish, Weight Watchers, and Zone Diets for weight loss and heart disease risk reduction: a randomized trial. JAMA. 2005;293:43-53.
35. Gardner CD, Kiazand A, Alhassan S, et al. Comparison of the Atkins, Zone, Ornish, and LEARN Diets for change in weight and related risk factors among overweight premenopausal women. The A TO Z Weight Loss Study: a randomized trial. JAMA. 2007;297:969-977.
36. Institutes of Medicine Food and Nutrition Board. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids. Washington, DC: National Academies Press; 2005. Available at https://nap.nationalacademies.org/read/10490/chapter/1. Last accessed January 16, 2024.
37. Tuomilehto J, Lindstrom J, Eriksson JG, et al. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N Engl J Med. 2001;344:1343-1350.
38. Diabetes Prevention Program Research Group. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. 2002;346:393-403.
39. Laaksonen DE, Lindström J, Lakka TA, et al. Physical activity in the prevention of type 2 diabetes: the Finnish Diabetes Prevention Study. Diabetes. 2005;54:158-165.
40. Sigal RJ, Kenny GP, Wasserman DH, Castaneda-Sceppa C, White RD. Physical activity/exercise and type 2 diabetes: a consensus statement from the American Diabetes Association. Diabetes Care. 2006;29:1433-1438.
41. Glasgow RE, Eakin EG, Fisher EB, Bacak SJ, Brownson RC. Physician advice and support for physical activity: results from a national survey. Am J Prev Med. 2001;21:189-196.
42. Centers for Disease Control and Prevention. Summary Health Statistics: National Health Interview Survey, 2015, Table A15. Available at https://ftp.cdc.gov/pub/Health_Statistics/NCHS/NHIS/SHS/2015_SHS_Table_A-15.pdf. Last accessed January 16, 2024.
43. Haskell WL, Lee IM, Pate RR, et al. Physical activity and public health: updated recommendations for adults from the American College of Sports Medicine and the American Heart Association. Circulation. 2007;116(9):1081-1093.
44. Nelson ME, Rejeski WJ, Blair SN, et al. Physical activity and public health in older adults: recommendation from the American College of Sports Medicine and the American Heart Association. Circulation. 2007;116(9):1094-1105.
45. Manson JE, Greenland P, LaCroix AZ, et al. Walking compared with vigorous exercise for the prevention of cardiovascular events in women. N Engl J Med. 2002;347:716-725.
46. Castaneda C, Gordon PL, Uhlin KL, et al. Resistance training to counteract the catabolism of a low-protein diet in patients with chronic renal insufficiency. Ann Intern Med. 2001;135:965-976.
47. Sjöström L, Rissanen A, Andersen T, et al. Randomised placebo-controlled trial of orlistat for weight loss and prevention of weight regain in obese patients. European Multicentre Orlistat Study Group. Lancet. 1998;352:167-172.
48. Finer N, James WPT, Kopelman PG, Lean ME, Williams G. One-year treatment of obesity: a randomized, double-blind, placebo-controlled, multicentre study of orlistat, a gastrointestinal lipase inhibitor. Int J Obes. 2000;24:306-313.
49. Hauptman J, Lucas C, Boldrin MN, Collins H, Segal KR. Orlistat in the long-term treatment of obesity in primary care settings. Arch Fam Med. 2000;9:160-167.
50. Apfelbaum M, Vague P, Ziegler O, Hanotin C, Thomas F, Leutenegger E. Long-term maintenance of weight loss after a very-low-calorie diet: a randomized blinded trial of the efficacy and tolerability of sibutramine—the Farmingham Study. Am J Med. 1999;106:179-184.
51. McMahon FG, Fujioka K, Singh BN, et al. Efficacy and safety of sibutramine in obese white and African American patients with hypertension: a 1-year, double-blind, placebo-controlled, multicenter trial. Arch Intern Med. 2000;160:2185-2191.
52. U.S. Food and Drug Administration. FDA Drug Safety Communication: FDA Recommends Against the Continued Use of Meridia (Sibutramine). Available at https://www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-communication-fda-recommends-against-continued-use-meridia-sibutramine. Last accessed January 16, 2024.
53. James WPT, Caterson ID, Coutinho W, et al. Effect of sibutramine on cardiovascular outcomes in over-weight and obese subjects.N Engl J Med. 2010;363:905-917.
54. Naghshizadian R, Rahnemai-Azar A, Kella K, et al. Patient perception of ideal body weight and the effect of body mass index. Journal of Obesity. 2014;(2014):491280.
55. Elder KA, Wolfe BM. Bariatric surgery: a review of procedures and outcomes. Gastroenterology. 2007;132(6):2253-2271.
56. American Society for Metabolic and Bariatric Surgery. Is Metabolic and Bariatric Surgery Right for You? Available at https://asmbs.org/patients/is-metabolic-and-bariatric-surgery-right-for-you/. Last accessed January 16, 2024.
57. Society of American Gastrointestinal and Endoscopic Surgeons. Guidelines for the Clinical Application of Laparoscopic Bariatric Surgery. Available at https://www.sages.org/publications/guidelines/guidelines-for-clinical-application-of-laparoscopic-bariatric-surgery. Last accessed January 16, 2024.
58. Sjöström L, Lindroos A, Markku P, et al. Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med. 2004;351:2683-2693.
59. Colquitt J, Clegg A, Loveman E, Royle P, Sidhu MK. Surgery for morbid obesity. Cochrane Database Syst Rev. 2005;2:CD003641.
60. Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA. 2004;292:1724-1737.
61. Christou NV, Sampalis JS, Liberman M, et al. Surgery decreases long-term mortality, morbidity, and health care use in morbidly obese patients. Ann Surg. 2004;240(3):416-423.
62. Adams TD, Gress RE, Smith SC, et al. Long-term mortality after gastric bypass surgery. N Engl J Med. 2007;357(8):753-761.
64. Fernandes M, Atallah AN, Soares BGO, et al. Intragastric balloon for obesity. Cochrane Database Syst Rev. 2007;1:CD004931.
66. Amaro A, Sugimoto D, Wharton S. Efficacy and safety of semaglutide for weight management: evidence from the STEP program. Postgrad Med. 2022;134 (S1):5-17.
67. Halaw H, Khemani D, Eckhart D, et al. Effects of liraglutide on weight, satiation, and gastric functioning in obesity: a randomized, placebo-controlled pilot study. Lancet Gastroenterol Hepatol. 2017;2(12):890-899.
68. Must A, Spadano J, Coakley EH, et al. The disease burden associated with overweight and obesity. JAMA. 1999;282(16):1523-1529.
69. National Heart, Lung, Blood Institute and North American Association for the Study of Obesity. The Practical Guide: Identification, Evaluation, and Treatment of Overweight and Obesity in Adults. NIH Pub. 00-4084. 2000. Available at https://www.nhlbi.nih.gov/files/docs/guidelines/prctgd_c.pdf. Last accessed January 16, 2024.
70. U.S. Department of Health and Human Services and Department of Agriculture. Dietary Guidelines for Americans, 2020–2025. Washington, DC: U.S. Department of Health and Human Services; 2020.
71. Lexicomp Online. Available at https://online.lexi.com. Last accessed January 16, 2024.
72. U.S. Food and Drug Administration. Meridia (Sibutramine Hydrochloride) Information. Available at https://wayback.archive-it.org/7993/20170406172234/https://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm191652.htm. Last accessed January 16, 2024.
73. Galuska DA, Will JC, Serdula MK, Ford ES. Are health care professionals advising obese patients to lose weight? JAMA. 1999;282(16):1576-1578.
74. Centers for Disease Control and Prevention. Summary Health Statistics for U.S. Adults: National Health Interview Survey, 2012. Available at https://www.cdc.gov/nchs/data/series/sr_10/sr10_260.pdf. Last accessed January 16, 2024.
75. Hales CM, Carroll MD, Fryar CD, Ogden CL. Prevalence of obesity and severe obesity among adults: United States, 2017–2018. NCHS Data Brief. 2020;360:1-7.
76. Mokdad AH, Marks JS, Stroup DF, Gerberding JL. Actual causes of death in the United States, 2000. JAMA. 2004;291(10):238-1245.
77. Speliotes EK, Willer CJ, Berndt SI, et al. Association analyses of 249,796 individuals reveal 18 new loci associated with body mass index. Nat Genet. 2010;42(11):937-948.
78. Bloss CS, Schork NJ, Topol EJ. Effect of direct-to-consumer genomewide profiling to assess disease risk. N Engl J Med. 2011;364(6):524-534.
79. Levi Z, Kark JD, Afek A, et al. Measured body mass index in adolescence and the incidence of pancreatic cancer in a cohort of 720,000 Jewish men. Cancer Causes Control. 2012;23(2):371-378.
80. Eliassen AH, Colditz GA, Rosner B, Willett WC, Hankinson SE. Adult weight change and risk of post-menopausal breast cancer. JAMA. 2006;296(2):193-201.
81. Whitmer RA, Gustafson DR, Barrett-Connor E, Haan MN, Gunderson EP, Yaffe K. Central obesity and increased risk of dementia more than three decades later. Neurology. 2008;71(14):1057-1064.
82. Thomas DE, Elliott EJ, Naughton GA. Exercise for type 2 diabetes mellitus. Cochrane Database Syst Rev. 2006;3:CD002968.
83. Centers for Disease Control and Prevention. How Much Physical Activity Do Adults Need? Available at https://www.cdc.gov/physicalactivity/basics/adults/index.htm. Last accessed January 16, 2024.
84. Halpern B, Faria AM, Halpern A. Bupropion/naltrexone fixed-dose combination for the treatment of obesity. Drugs Today (Barc). 2011;47(8):575-581.
85. Nguyen NT, Masoomi H, Magno CP, Nguyen XM, Laugenour K, Lane J. Trends in use of bariatric surgery, 2003–2008. J Am Coll Surg. 2011;213(2):261-266.
87. Mechanick JI, Kushner RF, Sugerman HJ, et al. American Association of Clinical Endocrinologists, The Obesity Society, and American Society for Metabolic and Bariatric Surgery Medical guidelines for clinical practice for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient. Endocr Pract. 2008;14(Suppl 1):1-83.
88. Nath A, Leblanc KA, Hausmann MG, Kleinpeter K, Allain BW, Romero R. Laparoscopic sleeve gastrectomy: our first 100 patients. JSLS. 2010;14(4):502-508.
89. Fuks D, Verhaeghe P, Brehant O, et al. Results of laparoscopic sleeve gastrectomy: a prospective study in 135 patients with morbid obesity. Surgery. 2009;145(1):106-113.
90. Jan JC, Hong D, Pereira N, Patterson EJ. Laparoscopic adjustable gastric banding versus laparoscopic gastric bypass for morbid obesity: a single-institution comparison study of early results. J Gastrointest Surg. 2005;9(1):30-39.
91. Tice JA, Karliner L, Walsh J, Petersen AJ, Feldman MD. Gastric banding or bypass? A systematic review comparing the two most popular bariatric procedures. Am J Med. 2008;121(10):885-893.
92. Boza C, Gamboa C, Perez G, et al. Laparoscopic adjustable gastric banding (LAGB): surgical results and 5-year follow-up. Surg Endosc. 2011;25(1):292-297.
93. Weghuber D, Barret T, Barrientos-Perez M, et al. Once-weekly semaglutide in adolescents with obesity. N Engl J Med. 2022;387:2245-2257.
94. Lincoff AM, Frandsen KB, Colhoun HM, et al. Semaglutide and cardiovascular outcomes in obesity without diabetes. N Engl J Med. 2023;389:2221-2232.
95. U.S. Food and Drug Administration. FDA Requests the Withdrawal of the Weight-Loss Drug Belviq, Belviq XR (Lorcaserin) From the Market. Available at https://www.fda.gov/drugs/drug-safety-and-availability/fda-requests-withdrawal-weight-loss-drug-belviq-belviq-xr-lorcaserin-market. Last accessed January 16, 2024.
96. Eisenberg D, Shikora SA, Aarts E, et al. 2022 American Society for Metabolic and Bariatric Surgery (ASMBS) and International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO) indications for metabolic and bariatric surgery. Obes Surg. 2023;33(1):3-14.
97. Mechanick JI, Apovium C, Brethauer S, et al. Clinical practice guidelines for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient—2019 update: cosponsored by American Association of Clinical Endocrinologists, The Obesity Society, American Society for Metabolic and Bariatric Surgery, Obesity Medicine Association, and American Society of Anesthesiologists. Endocrine Practice. 2019;25(12):1-75.
98. U.S. Food and Drug Administration. FDA Approves Weight-Management Drug Qsymia. Available at https://wayback.archive-it.org/7993/20170112130442/http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm312468.htm. Last accessed January 16, 2024.
99. U.S. Food and Drug Administration. FDA Approves Weight-Management Drug Contrave. Available at https://wayback.archive-it.org/7993/20170112222826/http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm413896.htm. Last accessed January 16, 2024.
100. Abid A, Galuska D, Khan LK, Gillespie C, Ford ES, Serdula MK. Are healthcare professionals advising obese patients to lose weight? A trend analysis. MedGenMed. 2005;7(4):10.
101. Bishop J, Middendorf R, Babin T, Tilson W. ASPE Research Brief: Childhood Obesity. Available at https://aspe.hhs.gov/basic-report/aspe-childhood-obesity-white-paper. Last accessed January 16, 2024.
102. Tsai AG, Williamson DF, Glick HA. Direct medical cost of overweight and obesity in the USA: a quantitative systematic review. Obes Rev. 2011;12(1):50-61.
103. O'Brien PE, MacDonald L, Anderson M, Brennan L, Brown WA. Long-term outcomes after bariatric surgery: fifteen-year follow-up of adjustable gastric banding and a systematic review of the bariatric surgical literature. Ann Surg. 2013;257(1):87-94.
104. American Society for Metabolic and Bariatric Surgery. Estimate of Bariatric Surgery Numbers 2011–2021. Available at https://asmbs.org/resources/estimate-of-bariatric-surgery-numbers. Last accessed January 16, 2024.
105. American Society for Metabolic and Bariatric Surgery. Studies Weigh in on Safety and Effectiveness of Newer Bariatric and Metabolic Surgery Procedure. Available at https://asmbs.org/resources/studies-weigh-in-on-safety-and-effectiveness-of-newer-bariatric-and-metabolic-surgery-procedure. Last accessed January 16, 2024.
106. Kosiborod MN, Abildstrom SZ, Borlaug BA, et al. Semaglutide in patients with heart failure with preserved ejection fraction and obesity. N Engl J Med. 2023;389:1069-1084.
107. U.S. Food and Drug Administration. FDA Approves New Medication for Chronic Weight Management. Available at https://www.fda.gov/news-events/press-announcements/fda-approves-new-medication-chronic-weight-management. Last accessed January 16, 2024.
108. Enright C, Thomas E, and Saxon DR. An updated approach to antiobesity pharmacology: moving beyond the 5% weight loss goal. Journal of the Endocrine Society. 2023;7(3):1-12.
109. U.S. Food and Drug Administration. FDA Approves Weight-Management Drug Saxenda. Available at https://wayback.archive-it.org/7993/20170111160832/http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm427913.htm. Last accessed January 16, 2024.
110. Ogden CL. Carroll MD, Lawman HG, et al. Trends in obesity prevalence among children and adolescents in the United States, 1988–1994 through 2013–2014. JAMA. 2016;315(21):2292-2299.
111. Locke AE, Kahali B, Berndt SI, et al. Genetic studies of body mass index yield new insights for obesity biology. Nature. 2015;518(7538):197-206.
112. Jensen MD, Ryan DH, Apovian CM, et al. 2013 AHA/ACC guideline for the management of overweight and obesity in adults. Circulation. 2014;129(25 Suppl 2):S102-S138.
113. Johnston BC, Kanters S, Bandayrel K, et al. Comparison of weight loss among named diet programs in overweight and obese adults: a meta-analysis. JAMA. 2014;312(9):923-933.
114. Yanovski SZ, Yanovski JA. Long-term drug treatment for obesity: a systematic and clinical review. JAMA. 2014;311(1):74-86.
115. Puzziferri N, Roshek TB, Mayo HG, et al. Long-term follow-up after bariatric surgery: a systematic review. JAMA. 2014;312(9):934-942.
116. World Health Organization. Obesity and Overweight. Available at https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight. Last accessed January 16, 2024.
117. U.S. Food and Drug Administration. The FDA Alerts Health Care Providers about Potential Risks with Liquid-Filled Intragastric Balloons. Available at https://wayback.archive-it.org/7993/20191216130206/https://www.fda.gov/medical-devices/letters-health-care-providers/fda-alerts-health-care-providers-about-potential-risks-liquid-filled-intragastric-balloons. Last accessed January 16, 2024.
118. U.S. Food and Drug Administration. ORBERA Intragastric Balloon System: P140008. Available at https://www.accessdata.fda.gov/cdrh_docs/pdf14/P140008c.pdf. Last accessed January 16, 2024.
119. U.S. Food and Drug Administration. FDA Approves First-of-Kind Device to Treat Obesity. Available at https://www.sciencedaily.com/releases/2015/01/150129170327.htm. Last accessed January 16, 2024.
121. Weihrauch-Bluher S, Schwarz P, Klusmann JH. Childhood obesity: increased risk for cardiometabolic disease and cancer in adulthood. Metabolism. 2019;92:147-152.
122. Kim DD, Basu A. Estimating the medical care costs of obesity in the United States: systematic review, meta-analysis, and empirical analysis. Value in Health. 2016;19:602-613.
123. Averginos KI, Spyrou N, Mantzoros CS, et. al. Obesity and cancer risk: emerging biological mechanisms and perspectives. Metabolism. 2019;92:121-135.
124. Tartof SY, Qian L, Hong V, et al. Obesity and mortality among patients diagnosed with COVID-19: results from an integrated health care system. Ann Int Med. 2020;173(10):773-781.
126. Heymsfield SB and Wadden TA. Mechanisms, pathophysiology, and management of obesity. N Engl J Med. 2017;376:254-266.
127. Courcoulas AP, Belle SH, Neiberg RH, et al. Three-year outcomes of bariatric surgery vs lifestyle intervention for type 2 diabetes mellitus treatment: a randomizes clinical trial. JAMA. 2015;150:931-940.
128. Pilitsi E, Farr OM, Polyzos SA, et al. Pharmacotherapy of obesity: available medications and drugs under investigation. Metabolism. 2019;92:170-192.
129. Ammon BJ, Skarulis MC, Soran H, et al. Medical and surgical management of obesity and diabetes: what's new? Diabetic Medicine. 2019;37:203-210.
130. Kelly AS, Auerbach P, Barrientos-Perez M, et al. A randomized, controlled trial of liraglutide for adolescents with obesity. N Engl J Med. 2020;382:2117-2128.
132. American Society for Metabolic and Bariatric Surgery. New Study Challenges Decades-old Patient Eligibility Criteria for Weight-loss Surgery. Available at https://asmbs.org/articles/new-study-challenges-decades-old-patient-eligibility-criteria-for-weight-loss-surgery. Last accessed January 16, 2024.
133. U.S. Food and Drug Administration. FDA Approves New Drug Treatment for Chronic Weight Management, First Since 2014. Available at https://www.fda.gov/news-events/press-announcements/fda-approves-new-drug-treatment-chronic-weight-management-first-2014. Last accessed January 16, 2024.
134. Wilding JPH, Batterham RL, Calanna S, et al. Once-weekly semaglutide in adults with overweight or obesity. N Engl J Med. 2021;384:989-1002.
135. U.S. Food and Drug Administration. FDA Approves Novel, Dual-Targeted Treatment for Type 2 Diabetes. Available at https://www.fda.gov/news-events/press-announcements/fda-approves-novel-dual-targeted-treatment-type-2-diabetes. Last accessed January 16, 2024.
1. U.S. Preventive Services Task Force. Behavioral weight loss interventions to prevent obesity-related morbidity and mortality in adults: U.S. Preventive Services Task Force recommendation statement. JAMA. 2018;320(11):1163-1171. Available at https://jamanetwork.com/journals/jama/fullarticle/2702878. Last accessed January 18, 2024.
2. Department of Veterans Affairs Management of Overweight and Obesity Working Group. VA/DoD Clinical Practice Guideline: Management of Adult Overweight and Obesity (OBE). Washington, DC: Department of Veterans Affairs, Department of Defense; 2020. Available at https://www.healthquality.va.gov/guidelines/CD/obesity/VADoDObesityCPGFinal5087242020.pdf. Last accessed January 18, 2024.
3. Eisenberg D, Shikora SA, Aarts E, et al. 2022 American Society of Metabolic and Bariatric Surgery (ASMBS) and International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO) indications for metabolic and bariatric surgery. Obes Surg. 2023;33(1): 3-14. Available at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9834364. Last accessed January 18, 2024.
Mention of commercial products does not indicate endorsement.