Over the years, the radiology department has evolved from a purely diagnostic area to one where multifaceted therapies are performed. Radiologists have evolved to become super-specialists, able to guide referring physicians to further tests and/or radiological therapies. The radiology residency now incorporates training in many areas that were unknown a few decades ago. Today, as patients spend a steadily increasing amount of time away from regular hospital units, they must be properly prepared for what is going to happen to them. The purpose of this course is to provide information about the rapidly expanding field of radiologic medicine. Knowledge of the basic procedures will assist physicians and nurses in preparing patients and their families for the many procedures performed in the radiology department.
- INTRODUCTION
- THE RADIOLOGY DEPARTMENT: A BRIEF SUMMARY
- THE SCOPE AND STAFF OF INTERVENTIONAL RADIOLOGY
- PATIENT SELECTION
- PATIENT PREPARATION
- MODERATE SEDATION
- A SYNOPSIS OF INTERVENTIONAL PROCEDURES
- ANGIOGRAPHY
- DIALYSIS FISTULA AND GRAFT REPAIR
- VASCULAR STENTS
- VASCULAR FILTERS
- CELIAC PLEXUS BLOCK
- INTENTIONAL EMBOLIZATION
- STENOSIS MANAGEMENT
- PERIPHERALLY INSERTED CENTRAL CATHETERS (PICC LINES)
- ENDOVASCULAR GRAFTS FOR ABDOMINAL AORTIC ANEURYSM REPAIR
- TRANSCATHETER HEART VALVE REPLACEMENT
- TRANSJUGULAR INTRAHEPATIC PORTOSYSTEMIC SHUNT
- TUMOR ABLATION
- INTERVENTIONAL INTRAVASCULAR DRUG THERAPY
- A NOTE ABOUT SAFETY
- THE ROLE OF THE NURSE
- CONCLUSION
- Works Cited
- Evidence-Based Practice Recommendations Citations
This course is designed for physicians, physician assistants, and nurses involved in the care of patients who may require radiological interventions.
The purpose of this course is to provide information about an expanding field of radiological medicine. Knowledge of the basic procedures will assist physicians and nurses in preparing patients and their families for the many procedures performed in the radiology department.
Upon completion of this course, you should be able to:
- Explain the indications and risks of interventional radiologic procedures and describe them to patients and their families.
- List measurable criteria to review before safely deciding to proceed with any interventional radiologic procedure.
- Discuss the factors involved in administering moderate sedation.
- Identify indications and outcomes for image-guided biopsy.
- Describe how drainage of obstructed organ systems or large fluid collections may be provided by percutaneous approaches.
- Discuss the methods by which percutaneous nephrostomy and ureteral stents aid in the treatment of urologic disease.
- Review the role of interventional procedures in establishing drainage of the biliary system.
- Describe indications for and possible complications resulting from various angiography procedures.
- Summarize the proper placement of vascular stents and filters.
- Discuss the use of celiac plexus block, including expected outcomes.
- Identify conditions that warrant the use of intentional embolization.
- Review the mechanism of action and objectives of radiofrequency tumor ablation.
- List side effects and contraindications of interventional intravascular drug therapy.
Linda Strangio, RN, MA, CCRN, CRN, graduated from The Mount Sinai Hospital School of Nursing in New York City. Linda has been a staff nurse, head nurse and patient care coordinator in medical, surgical and pulmonary intensive care units in New York, Ohio and New Jersey. In 1992, she became the nursing coordinator of the department of radiology at Atlantic Health System's Mountainside Hospital in Montclair, New Jersey, where she had worked for twenty-six years. She held national certification in critical care nursing (CCRN) and radiology nursing (CRN), as well as two degrees in psychology. She was the editor of Images, which is the national journal of the American Radiological Nurses Association (ARNA), has been published over fifty times in professional journals and magazines and has authored three books. Regrettably, Linda Strangio passed away in October 2002.
Contributing faculty, Linda Strangio, RN, MA, CCRN, CRN, has disclosed no relevant financial relationship with any product manufacturer or service provider mentioned.
John M. Leonard, MD
Jane C. Norman, RN, MSN, CNE, PhD
The division planners have disclosed no relevant financial relationship with any product manufacturer or service provider mentioned.
Sarah Campbell
The Director of Development and Academic Affairs has disclosed no relevant financial relationship with any product manufacturer or service provider mentioned.
The purpose of NetCE is to provide challenging curricula to assist healthcare professionals to raise their levels of expertise while fulfilling their continuing education requirements, thereby improving the quality of healthcare.
Our contributing faculty members have taken care to ensure that the information and recommendations are accurate and compatible with the standards generally accepted at the time of publication. The publisher disclaims any liability, loss or damage incurred as a consequence, directly or indirectly, of the use and application of any of the contents. Participants are cautioned about the potential risk of using limited knowledge when integrating new techniques into practice.
It is the policy of NetCE not to accept commercial support. Furthermore, commercial interests are prohibited from distributing or providing access to this activity to learners.
Supported browsers for Windows include Microsoft Internet Explorer 9.0 and up, Mozilla Firefox 3.0 and up, Opera 9.0 and up, and Google Chrome. Supported browsers for Macintosh include Safari, Mozilla Firefox 3.0 and up, Opera 9.0 and up, and Google Chrome. Other operating systems and browsers that include complete implementations of ECMAScript edition 3 and CSS 2.0 may work, but are not supported. Supported browsers must utilize the TLS encryption protocol v1.1 or v1.2 in order to connect to pages that require a secured HTTPS connection. TLS v1.0 is not supported.
The role of implicit biases on healthcare outcomes has become a concern, as there is some evidence that implicit biases contribute to health disparities, professionals' attitudes toward and interactions with patients, quality of care, diagnoses, and treatment decisions. This may produce differences in help-seeking, diagnoses, and ultimately treatments and interventions. Implicit biases may also unwittingly produce professional behaviors, attitudes, and interactions that reduce patients' trust and comfort with their provider, leading to earlier termination of visits and/or reduced adherence and follow-up. Disadvantaged groups are marginalized in the healthcare system and vulnerable on multiple levels; health professionals' implicit biases can further exacerbate these existing disadvantages.
Interventions or strategies designed to reduce implicit bias may be categorized as change-based or control-based. Change-based interventions focus on reducing or changing cognitive associations underlying implicit biases. These interventions might include challenging stereotypes. Conversely, control-based interventions involve reducing the effects of the implicit bias on the individual's behaviors. These strategies include increasing awareness of biased thoughts and responses. The two types of interventions are not mutually exclusive and may be used synergistically.
#90444: A Review of Interventional Radiology
It is probably safe to say that the world of medicine changes more rapidly than most other disciplines. Much of what is part of our daily routine today was no more than a dream a generation ago. Perhaps more than other medical specialties, radiology has grown faster and become more complex. It enables us to see inside the body and allow minimally invasive sampling and treatment of body structures and organ systems with greater precision.
In the past, the field of radiology had been one of uncertainty for personnel in other areas of the hospital. Patients left their hospital rooms for procedures the staff might have known little about. Outpatients were sent to the radiology department by their attending physicians to undergo tests that often seemed strange or frightening. At times, only the radiology personnel were able to explain the procedures. This has changed significantly, but we should all continue to update our knowledge of what the procedures entail so that we can explain them to our patients and their families.
The radiology department has evolved from a purely diagnostic area to one where multifaceted therapies are performed. Patients no longer visit the x-ray department simply to have x-rays taken. Radiologists have evolved to become super-specialists, able to guide referring physicians to further tests and perform many types of therapeutic procedures. Radiologic technicians have lengths of study and clinical experiences equal those of many nursing students and their knowledge of, and expertise with, anatomy and physiology is superb. Because the radiology department is usually staffed mainly with technologists, not nurses, technologists learn and perform basic nursing care and function as extensions of the nurse while the patient is in the department. The American Radiological Nurses Association (ARNA) is recognized by the American Nurses Association as a true specialty with its own certifying exam. Nationally certified radiology nurses use the credential "certified radiological nurse" (CRN). As patients spend an increasing amount of time away from regular hospital units, they should be properly prepared and educated for what is going to happen to them.
In this course, several of the procedures performed in the radiology department will be discussed, specifically those performed by interventional radiologists. This course is meant to provide a review to those with an understanding of radiologic procedures and to provide an overview to those for whom the subject may be new.
Some of the descriptions, tables, and illustrations that follow may seem simplified or overly detailed, such as how patients are positioned for studies; however, some patients or practitioners may wish, or need, to know this information. For these reasons, more detail, even if simplified, is included in this course.
In November 1895, Wilhelm Röntgen, a physics professor at the University of Würzburg in Germany, discovered the x-ray. First called the X-light, Röntgen's discovery earned him the first Nobel Prize for physics. Since those early days, the field of radiology has advanced steadily from crude unprotected picture-taking by "skiagraphers" to a complex and intricate arena driven by sophisticated, state-of-the-art computer technology. Now, more than 100 years later, radiology departments and imaging centers have opened windows into the body, allowing for treatment and intervention in addition to diagnosis [1].
Most radiology departments are subdivided according to imaging modalities, as shown in Table 1. Although variations exist, certain standards are basic and the areas usually remain as one department. Required patient procedures should be devised by radiology department staff and communicated to nursing units, clinics, and referring physicians' offices. It is essential for all sections of the radiology department to remain in contact to render proper care. For example, a computed tomography (CT) scan of the abdomen should be performed before a gastrointestinal (GI) series so the accumulated barium will not block the subtle detail seen on the CT scan. Incorrect scheduling or improper preparation may delay diagnosis and therapy and add days to the patient's length of stay.
COMMON RADIOLOGY STUDIES
| Type of study | Examples | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Diagnostic x-ray studies |
| ||||||||||||||
| MRI |
| ||||||||||||||
| Ultrasound (sonography) |
| ||||||||||||||
| CT scanning |
| ||||||||||||||
| Nuclear medicine (may be a separate department) |
| ||||||||||||||
| Interventional radiology |
|
Diagnostic radiology has historically been the backbone of any radiology department. In this area, general imaging techniques are employed and the most patients are seen. Procedure times range from just a few minutes (e.g., chest x-ray) to several hours (e.g., small bowel series), and from simple to complex. From automobile accidents to kidney stones and from strokes to abdominal pain, the diagnostic x-ray department is where it all starts. Initial screening is performed here, as are more sophisticated and more detailed procedures.
It is in this hospital department that many patients are given barium orally or rectally or have dyes and contrast agents instilled via tubes or drains to outline specific wound sites or follow the resolution of an abscess. They may receive intravenous x-ray contrast or have it injected through various fistulas or stomas. The diagnostic x-ray division has a rapid patient turnover, and the results often guide the next step, whether it be further testing or curative treatment.
It is important to note which dyes or contrast media have been used in the initial studies so that they may be considered prior to beginning more advanced or detailed procedures.
Rather than using x-rays to develop still images on a film that required processing time, early 20th century Edison fluoroscopes projected x-rays through the target and onto a tungsten metal-salt coated screen that fluoresced when excited by various levels of radiation, thereby producing a live-action image. The radiologist would sit behind the viewing screen, directly in the radiation field. Soon after the invention of television, TV cameras were the eyes behind the fluorescent screen. In modern fluoroscopes, x-rays are passed through the target and are collected by a phosphor intensifier, then digitally recorded and transmitted as moving images to a viewing screen. Contrast agents are used to enhance studies of soft tissues.
In the past, fluoroscopy was thought to be safe enough to use for shoe fitting in footwear stores. That proved to be incorrect. The medical benefit of fluoroscopy, however, outweighs the risks of prolonged x-ray exposure (e.g., radiation burns, cancer) [2]. Many newer devices allow for pulsed radiation and freeze-frame viewing, reducing radiation exposure to the patient and the staff.
Formerly known as computerized axial tomography (CAT), the newer machines employ various imaging methods that allow the clinician to view cross-sectional and three-dimensional images of the body through scans taken from different angles and varying depths. The newer CT scanners are more patient friendly. The patient lies on a table that is moved into the center of the scanner. After the camera is positioned, the x-ray tube moves around the opening as it obtains images. The scanner takes a series of rapid readings, then a computer generates an exact model of the area, showing excellent detail [3].
The CT scanner is an extremely fast machine compared to magnetic resonance imaging (MRI). Its ability to produce images of the body with great precision has revolutionized competency and speed of diagnosis and often gives an immediate answer to the question of what is happening in areas of the body that routine x-rays cannot see. Emergency departments rely heavily on the CT scanner to aid in the diagnosis of many patients; in fact, many emergency departments have their own units. Patients who undergo CT scanning of the abdomen and/or pelvis often ingest a barium type solution to highlight the digestive tract. Most patients are also given an iodine-based intravenous contrast injection that enhances the images and shows details of suspicious areas that otherwise might be missed. Some estimates of the number of intravascular administrations of a radio-opaque contrast medium exceed 10 million procedures per year in the United States alone. Of this number, a relatively large percent of exams are in the area of CT scanning.
One benefit of MRI is that it is accomplished without the use of x-rays. The old name, nuclear magnetic resonance, was dropped because this modality has nothing to do with radioactivity and the word "nuclear" frightened some patients. The process involves a large, powerful magnet, radiofrequency (nonionizing) emissions, and computer analysis [4].
In simplest terms, when the human body is placed in a strong magnetic field, hydrogen atoms and molecules inside the body are affected. The computer picks up the movement and converts it to a very detailed image.
The first MRI units were closed magnets that were shaped like tunnels, with openings on both ends and open spaces in the sides. However, an increasing number of new MRI units are more open, making them less uncomfortable for the patient. The quality of most of these scanners comes close to that of the tunnel-like units. An average test may take anywhere from 20 minutes to one hour or more. While the scan is in progress, a loud banging noise is usually audible to the patient, which is caused by the equipment and changing magnetic fields.
Because of the strong magnetic field, no objects that can be attracted by a magnet can be brought into the MRI room, and there are various relative and absolute contraindications for the examination. The magnet may affect devices such as cardiac pacemakers, internal defibrillators, and implanted nerve stimulators unless the devices are specifically magnetic resonance (MR) conditional. MR conditional devices allow patients to safely undergo MRI as long as the machine is correctly calibrated. However, so patients with non-MR-conditional devices are excluded from undergoing MRI exams. The same holds true for most aneurysm clips because the magnetic field may cause some of them to move or twist, an event that could prove catastrophic. Therefore, before beginning any MRI exam, patients should fill out a detailed medical history form for their protection. MRI provides detailed anatomic images, and it is excellent for the diagnosis of soft tissue abnormalities.
Many studies are enhanced by the intravenous injection of contrast agents that are specific for MRI examinations. These are commonly dyes based on gadolinium, a paramagnetic, rare-earth chemical element. In 2006, the U.S. Food and Drug Administration (FDA) issued a public health advisory regarding gadolinium-based contrast agents (GBCAs) because of the development of nephrogenic systemic fibrosis (NSF) in 25 patients with acute or chronic severe renal insufficiency; by December 2006, 69 cases were reported to the FDA [5,6]. The advisory has since been updated, and the FDA has mandated a boxed warning describing the risk of NSF on all nine GBCAs available in the United States [7,8]. The 2010 update states that GBCAs increase the risk for the development of NSF among patients with severe renal insufficiency or renal dysfunction. The FDA has not received reports of NSF among patients with normal renal function or moderate renal insufficiency [7]. The symptoms of NSF are [7,9,10]:
Swelling, hardening, and tightening of the skin
Reddened or darkened patches on the skin
Burning or itching of the skin
Yellow raised spots on the whites of the eyes
Stiffness in the joints or problems moving or straightening arms, hands, legs, or feet
Pain deep in the hips or ribs (diaphragm)
Muscle weakness
There is presently no treatment for NSF, which worsens over time and can cause death; however, kidney transplantation can slow or halt the condition [7].
In 2015, the FDA began investigating the risk of deposits of GBCAs in the brains of some patients following repeated use of GBCAs [8]. The investigation is based on reports in the literature that specifically site GBCA deposits in the brains of some patients who had undergone four or more contrast MRI scans. The deposits appeared long after the last administration of the contrast agent. In 2017, the FDA began requiring a new class warning and other safety measures for all GBCAs for MRI concerning gadolinium remaining in patients' bodies, including the brain, for months to years after receiving these drugs [11]. The retention of gadolinium has not been directly linked to adverse health effects in patients with normal kidney function, and the agency concluded that the benefit of all approved GBCAs continues to outweigh any potential risks [11,12]. In addition to approving the updated prescribing information concerning gadolinium retention, the FDA also approved new patient Medication Guides for all GBCAs. MRI centers should provide a Medication Guide the first time an outpatient receives a GBCA injection or when the information is substantially changed [11]. The FDA continues to recommend that healthcare professionals consider limiting GBCA use to clinical circumstances in which GBCA use provides additional, necessary information [8].
Ultrasonography exams use sound waves to form images. The basic principle is the same as that of sonar or depth sounding in studies of the ocean. In diagnostic ultrasonography, the ultrasonic waves are produced by electronically stimulating a crystal transducer. After applying a small amount of a jelly-like substance over the area to be scanned, the technologist moves a transducer across the site. As the beam strikes an interface or boundary between tissues of varying density, such as blood and muscle, some of the sound waves are reflected back to the transducer as echoes. The echoes are converted into electrical impulses that present an image of the tissues under examination [9].
Ultrasound can be used to examine many areas of the body. Blood flow can be observed using color Doppler techniques as it courses through the veins, arteries, and heart. Normal and pathologic tissues can be seen, and fluid collections in the body cavities can be clearly demonstrated. Ultrasound can measure sizes and shapes of various organs and is very valuable as an aid in obstetrics and gynecology, where x-rays should be avoided. The technique can evaluate fetal size and maturity and fetal and placental position. It is also a fast, relatively safe, and reliable technique to diagnose multiple pregnancies. Aside from drinking a copious amount of water for scans in the pelvic region, there is no real preparation needed. Ultrasonography is painless and noninvasive, with the exception of transvaginal or transrectal probes that are sometimes used. For this reason, ultrasound is often the first exam ordered, in the hope of achieving a diagnostic answer as quickly and safely as possible. Ultrasound can diagnose tumors, aneurysms, and a vast array of disorders. An advance in ultrasound is 3-D imaging, which can convert still images into a lifelike display.
Concern has been expressed about the overuse of high-power 3-D ultrasound imaging and fetal exposure to high energy levels, especially in nonmedical settings. Some studies have shown that higher rates of conventional low-power prenatal ultrasound exposure to the fetus may be associated with delayed speech, increased incidence of left-handedness, fetal growth restriction, and low birth weight [13,14,15]. The FDA has recommended that all keepsake 3-D and 4-D (movie type) ultrasonography be avoided due to effects on the fetus [16,17]. It is recommended that prenatal ultrasound should be limited to brief exposure and only when medical benefit will be derived [16].
Although it is occasionally a separate department, the nuclear medicine section uses radioisotopes for diagnostic and therapeutic purposes. These compounds are given orally or intravenously and are tracer agents for the areas to be studied. The tissue targeted "picks up" the injected isotope, which is then tracked by imaging or scanning equipment. In that regard, nuclear medicine differs from diagnostic radiology; the radiation is within the patient and is detected by the external device. Although the administered materials are radioactive, they are very low level and are excreted safely and quickly from the body. Some tests are carried out immediately after the injection, but others require a wait of several hours or even days because various agents take different amounts of time to get to and settle in the areas or organs being studied.
Patients are usually scanned while lying down or sitting adjacent to a scintillation camera. Nuclear medicine studies can detect tumors, fractures, abscesses, arthritis, bleeding points, ischemic cardiac regions, and a multitude of other problems. Importantly, besides structure, these tests usually illustrate how the organs function. For example, renal scans show the structure and function of the kidneys and may be enhanced by giving certain medications during the studies. Lung scans detect emboli and other lesions by showing perfusion, which illustrates regional blood flow to the lungs, and ventilation, which compares it to airflow. For this test, the patient inhales a radioactive gas to show ventilation and also receives an intravenous injection to outline pulmonary perfusion. Nuclear cardiology studies, in which various types of cardiac scans are performed, have become very popular. For example, the exams can show perfusion of the heart muscle before and after increased stress caused by treadmill exercise or induced by inotropic drugs. Studies are available to image the functioning of brain tissue (e.g., positron emission tomography [PET] scanning), which has become an important step in attempting to diagnose Alzheimer disease [18].
After their diagnostic procedures, patients need not take any special precautions and are not considered to be significantly radioactive. Half-lives of these agents are short, but patients may be encouraged to drink extra fluids to minimize the amount of contact the isotopes have with the urinary bladder. Some patients may be advised not to hold small infants until the radioactive tracer is out of their system.
Known as the operating room of the radiology department, interventional radiology has expanded greatly. Sometimes referred to as the special procedures division, interventional radiology is staffed by personnel trained to conduct invasive procedures, biopsy deep internal organs, drain abscesses and cysts, open blocked arteries and veins with devices or medications, and provide a means by which obstructed kidneys and biliary tracts may be emptied. Rather than an area of screening, interventional radiology is usually where patients end up for therapeutic procedures, often after several other diagnostic studies.
For example, a patient with abdominal pain and jaundice may have undergone extensive x-rays, ultrasound, CT, MRI, and biliary scans, only to find him or herself on the interventional radiology table undergoing a percutaneous transhepatic cholangiogram that will drain blocked bile ducts and relieve symptoms. It is this area of practice that has revolutionized much of patient care and treatment and is the basis for the material contained in this course. The remainder of this course will focus on the types of procedures performed and their associated benefits and possible disadvantages.
The Society of Interventional Radiology (SIR) estimates that there are more than 8,000 interventional radiologists in the United States. According to the Society, advantages of interventional radiology include [19]:
The ability to perform most procedures in an outpatient setting
General anesthesia is usually not required
Risk, pain, and recovery time are often significantly reduced
The procedures are sometimes less expensive than surgery
Interventional radiology is usually performed in a designated section within the radiology department. As noted, much more than just a diagnostic area, interventional radiology areas function as minor operating rooms. Because special procedure radiography may pose a risk to the patient, hemodynamic and cardiac monitoring devices are standard, as is an array of emergency equipment and medications. Most institutions differentiate between cardiac angiography laboratories and those used for general interventional angiography. The material covered in this course excludes cardiac angiography and associated procedures. The need for a dedicated interventional radiography suite depends on the size of the institution and the number and types of procedures performed. For example, nonvascular special procedures do not need quite the same equipment as those involved with invasive neuroradiology. However, as with all aspects of the radiology department, the divisions remain intertwined and continue to rely upon each other for backup and support.
In an area as specialized as this, there is a need for expert personnel. Interventional radiologists actually perform these invasive procedures and may further specialize to even sharper delineated areas of expertise. For example, the physician who biopsies livers is not always the one who performs the balloon angioplasties and stent insertions. Again, the scope of practice depends on the individual institution and the level of medical expertise available.
At the heart of the interventional radiology team, in addition to the physicians, are its special-procedures technologists, many of whom have become certified and specialized in cardiovascular interventional radiology. These technologists have extensive knowledge of the anatomy and technical requirements and are true experts in their fields.
The interventional radiology nurse is a vital member of the team and is responsible for patient care during a procedure. Although assisting with a procedure is part of the role, the radiology nurse's primary function in the room is to monitor and assess the patient so that safe and effective care is continually provided. The radiology nurse should have a critical care background, as he or she is responsible for observing cardiac rhythms, monitoring changes in monitoring patterns, and administering various medications. The nurse should also be certified in IV therapy and cardiopulmonary resuscitation (CPR). Most procedures are performed under local anesthesia with IV moderate sedation, and this also falls within the scope of radiology nursing.
Almost all interventional radiologic procedures are carried out in the special fluoroscopy suite fitted with elaborate monitoring and recording equipment, power contrast injectors, electrical supplies, and built in oxygen, suction, and ventilator outlets. The use of fluoroscopy is essential as it allows the operator to follow the course of the procedure as it progresses. Nonvascular procedures may be performed in the CT or ultrasound departments. These complementary studies are useful in localizing masses or anatomic sites.
Interventional radiology provides services that were once performed only in operating rooms. Many physicians remember when patients were routinely sent to surgery for exploratory laparotomies under general anesthesia and returned after having had an open and close with biopsy. Although this may still occasionally be found, an increasing percentage of these cases are performed in the radiology suite as same day procedures. Tumors are pinpointed by CT scan or with ultrasound guidance and a sample of tissue is obtained by needle biopsy. The pathologist is able to tell whether the mass is a primary lesion with a good chance of resection, a lesion from a distant metastasis, or an inflammatory process. When all the information is in, the healthcare team is able to advise the patient and family of the best treatment options. In this way, many unnecessary and more invasive procedures can be avoided.
Major bypass grafting procedures comprise a large part of any operating room schedule. In many cases, this means opening the abdomen and constructing means for a new blood supply to areas deprived of circulation. Now, however, not all patients with occluded arteries are routinely scheduled for these surgeries. There are a great number of patients who can be helped by angioplasty, such as in balloon angioplasty, whereby the balloon catheter is inserted through the femoral artery and maneuvered to the point of stenosis. In some cases, stent insertion follows this angioplasty, giving extra insurance that the area remains patent. These procedures are performed in the interventional radiology suite, allowing most patients to go home either the same day or the following morning.
As mentioned, interventional radiology procedures can open occluded grafts, drain large abscesses, and puncture cysts. They provide radiographic guidance so that stents and shunts may be inserted to allow body fluids to escape through once-blocked natural pathways. The great advantage of interventional radiology is that all this is accomplished without open surgery and without major insult to organ systems resulting from a lengthy procedure. Patients are spared the discomfort and inconvenience of a myriad of possible post-surgical complications. In addition, the increasing possibility of contracting nosocomial infections is diminished.
Hospitals are under growing pressure to shorten length of stay; interventional radiology does exactly that. Minimal recuperation time is needed, and aside from possible minor pain, patients usually feel quite well the following day. Interventional radiology is a cost effective and relatively comfortable, patient-centered alternative to something most people do not want, provided in a manner that works for almost everybody.
While every effort is made to avoid subjecting patients to long and involved interventions, not every patient is a candidate to be discharged the day of or even the day following a procedure. In certain instances, patients should be observed and followed for longer periods. Certain types of drainages and IV drug administration, for example, require serial imaging, with therapy dependent on the results of what is found. Patients should be evaluated on an individual basis so that they receive maximum benefit.
Even if a patient remains under observation in the hospital, it should be remembered that by using the short-stay procedure itself, the patient has been spared a longer and usually more invasive hospitalization. Institutions do, of course, vary in their policies. Some facilities discharge patients just a few hours after balloon angioplasty, while others keep them overnight. These interventional radiologic procedures are still called short-stay procedures; the term encompasses those that limit the time patients spend in the hospital.
Inpatients, of course, have the same types of services available to them. After their procedures are completed, they return to their own nursing units and are monitored there instead of in the same day surgery area. It is often a pleasant and unexpected surprise for them and their families to learn that they are going to be treated in the radiology department instead of the operating room.
Obviously, not every patient is a candidate for an invasive procedure, no matter how minor it may be considered. Biopsies are performed using long sampling needles that are often inserted into organs deep within the body. For many reasons, patients should be evaluated before any decision is made to proceed. Blood work should be obtained and the results reviewed to assure that platelet counts, prothrombin time (PT), international normalized ratio (INR), and activated partial thromboplastin time (PTT) are within normal limits. The liver and kidney, for example, are two highly vascular organs, and patients with bleeding or clotting dysfunctions may be considered too much of a risk to undergo needle biopsy.
There are many patients with peripheral vascular disease who could benefit greatly from an interventional radiologic procedure but are on some type of anticoagulant. Many of these are inpatients who are receiving heparin drips. While most physicians feel it is adequate to stop the medication four hours before the procedure is to begin, some feel the lab work should be repeated immediately before the procedure begins. Others may believe this is unnecessary. The effective half-life of heparin is about 90 minutes, so the four-hour window seems to provide more than an adequate margin for safety [20].
Outpatients who take a vitamin K antagonist (VKA) (e.g., warfarin) on a daily basis are usually told to lower or stop their medication four to seven days before the date of the scheduled procedure because the effective half-life of warfarin is measured in days [20,21]. Blood work is drawn before the test, and the case proceeds if the INR has dropped satisfactorily. In recent years, use of the INR has replaced monitoring of prothrombin time and has been adopted as the world standard for monitoring VKA therapy. In general, the INR should be less than 1.5 or 1.7 prior to any invasive procedure to prevent bleeding [21,22]. For the same reason, platelet counts should not be below 50,000/mm3. Certain over-the-counter medications, such as aspirin, can also cause anticoagulation, so a complete drug history should be taken when patients are being interviewed. The patient's use of alternative or herbal medications should also be reviewed.
It is extremely important to conduct a complete assessment before any invasive procedure is performed. As noted, no matter how minor it may be considered, an invasive procedure involves something physically entering the patient's body. If the same diagnostic information can be gained by similar but noninvasive techniques, the radiologist should thoroughly discuss this with the referring physician. With the area of radiology so specialized, it is not realistic to believe that every exam ordered by a general internist or other clinician is the optimal one for that patient. In many facilities, for example, angiographies are only performed after consultation with a vascular surgeon. Biopsy requests should be approved by the radiologist reviewing the films to assure that the lesion or site requiring sampling is safely accessible by the long biopsy needles.
The Kidney Disease: Improving Global Outcomes (KDIGO) Work Group recommends assessing the risk for contrast-induced acute kidney injury and, in particular, screening for pre-existing impairment of kidney function in all patients who are considered for a procedure that requires intravascular (or intra-arterial) administration of iodinated contrast medium. Alternative imaging methods should be considered in patients at increased risk for contrast-induced acute kidney injury.
(https://kdigo.org/guidelines/acute-kidney-injury Last Accessed: June 1, 2022)Level of Evidence: Expert Opinion/Consensus Statement
Another area to be assessed is renal function. Almost all radiologic images are enhanced by the administration of intravenous or intra-arterial contrast agents. Many of these agents, except for those used in MRI, are iodinated. All contrast compounds enhance the images and show details of specific areas that otherwise might easily be missed. As we know, during angiography the injected contrast material provides a detailed map of the vessels themselves and depicts the paths of blood flow. The contrast material remains visualized until significant hemodilution occurs. Most procedures cannot be performed without some type of intravascular contrast agent.
The conventional ionic contrast materials, such as diatrizoate, iothalamate, and metrizoate, are monomeric salts of tri-iodinated benzoic acid [20]. The anion is the radiopaque portion, but because the anion and cation are osmotically active, the agent is significantly hypertonic to plasma. The tonicity of the solution is five to eight times the tonicity of plasma. This hypertonicity is a major cause of the side effects seen with these agents [23].
The low osmolar, nonionic contrast agents such as metrizamide, iopamidol, and iohexol are also tri-iodinated. However, they do not dissociate in solution and hypertonicity does not occur. Side chains have been altered, which makes the molecule more soluble without dissociation [23]. This reduces the side effects dramatically, but the cost of these agents may be nearly 10 times the cost of the ionic contrast media. Some procedures, such as myelography, cannot be performed with the ionic agents, making the nonionics the necessary materials.
As noted, the various types of x-ray contrast materials are all either ionic or nonionic when broken down to their simplest form. Both types contain iodine, which may be considered potentially nephrotoxic, as the dye has an acute osmotic effect that can further compromise function due to its dehydrating properties. Injection of a contrast medium produces an initial vasodilatation, which is followed by a reactive vasoconstriction in the renal circulation, an effect implicated in renal toxicity. X-ray dye is administered cautiously to patients with renal insufficiency; blood urea nitrogen (BUN) and creatinine levels should always be checked [23,24]. A BUN greater than 23 mg/dL or a creatinine greater than 1.2 mg/dL should signal a warning to be careful.
Patients suffering from congestive heart failure may also show adverse effects from IV contrast materials as they expand vascular volume and increase blood return to the right side of the heart [24]. The FDA warns of small but serious risks associated with iodinated contrast media including kidney damage and anaphylaxis [7]. Patients with multiple myeloma have a significant potential for kidney damage after iodinated contrast injection because the dye may potentiate the precipitation of protein in the kidney [24]. An oral diabetic agent, metformin, has been shown to have a small potential to cause renal damage if given with iodinated x-ray contrast agents due to the possibility of lactic acid formation [24]. This problem may be avoided by discontinuing the metformin for two days after the contrast material is given and being certain renal function is adequate before restarting the drug. In each case, a complete medical assessment should be completed and the decision made whether the benefit of the procedure outweighs any potential harm to the patient before any procedure using contrast materials is performed.
Some patients present with a history of previous reaction to contrast agents. In those instances the true nature of the previous episode should be ascertained. While a mild reaction to an iodinated contrast medium is not uncommon, serious adverse reactions must be avoided. Some common reactions are listed in Table 2. Most instances of adverse reactions are due to high osmolar (ionic) iodinated contrast media.
CLASSIFICATION OF CONTRAST AGENT REACTION
| Mild | Moderate | Severe | ||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
|
Nonionic iodinated CT contrast media are associated with a very low incidence of adverse reactions. A review of 298,491 doses given at a single facility over the course of four years shows that the most common adverse reactions to these agents (498 total) are hives and nausea; most required no treatment; 79 required treatment in the radiology department, and 16 of those 79 required outside treatment—one death occurred 30 minutes after media injection [25]. Additionally, 32 of the 79 incidents were in patients who had previous allergies to contrast media and had received premedication, 2 of which required further treatment in the emergency department [25]. Patients may be premedicated with diphenhydramine (Benadryl) and one of the corticosteroids (generally reserved for patients with previous moderate or severe idiosyncratic adverse reactions) [23]. Table 3 is an example of one possible premedication protocol.
SAMPLE OF PREMEDICATION POLICY OF PATIENTS WITH KNOWN CONTRAST AGENT SENSITIVITY
Diphenhydramine 50 mg given orally or IV 1 hour prior to procedure. Have available all necessary resuscitation equipment. |
Even though the cost of low osmolar (nonionic) intravenous contrast materials has gone down, they are still more expensive than ionic contrast agents. Despite the higher cost, most facilities use nonionic contrast materials because of increased patient comfort and satisfaction, decreased adverse reactions, and fewer hospitalizations, making them more cost effective [25,27].
Because most patients undergoing short-stay procedures are sent home the same day, it is vital to adhere to the criteria developed for these patients. First, the patient should know what to expect before he or she arrives in the department. For patients to cooperate, they must understand what to expect. The referring physician should explain to the patient what the procedure entails and why it is being performed. Many patients have no idea why something is indicated. When asked, most simply say that it is because their doctor prescribed it. Patients need initial information from their own doctor or healthcare provider.
In some facilities, the radiology nurse or special procedures (interventional radiology) scheduler calls the patient at home to set up the procedure. In other facilities, patients are asked to come to the hospital for their preprocedure assessment. This is the optimal time for the radiology staff to interview the patient, being certain to obtain a complete medical and surgical history. A list of medications currently being taken, any allergies, and any other pertinent information should be recorded and kept on hand for the day the procedure is performed. Most institutions use a checklist for the initial screening and follow up when the patient arrives in the department. Secretaries refer patients to the radiology nurse with questions about such things as insulin diuretic use, or allergies.
Most facilities tell their patients not to eat or drink anything after midnight, but some allow the patient to have a clear liquid breakfast. Before angiography, patients may be told to drink several glasses of water to protect against the dehydrating effects of the intravascular contrast material. This first interview is the time for a quick review of what is going to happen. Patients and families should be given a telephone number to call if they think of any questions between the interview and the test. Just knowing there is someone available can be reassuring.
Patients who undergo same-day procedures should be cooperative and reliable. They should have someone drive them home from the hospital, and they should not be alone in their homes overnight. These two standards should be followed and are strict prerequisites for same-day discharge. This is necessary so that they are not alone if any complications should develop. There are some patients who do not mind being kept overnight in the hospital, but they should understand that some insurance companies will not cover their hospital costs. When patients first arrive at the hospital, they should state who is going to take them home and with whom they will be spending their post-procedure night. When all is in order, the immediate preparation may begin.
Naturally, hospitals vary in the way patients are admitted, but in general, the procedures are similar. The patient's family or significant other is invited to accompany the patient as the interventional radiologist and radiology staff will meet with him or her and explain the details of what is to be performed, including the risks and potential complications of the procedure. This is the time for any further questions to be addressed and the informed consent form signed and witnessed; however, ideally it would be completed the day before the procedure. A complete review of any prior radiologic procedures should be made. The day of the procedure, the patient is admitted and standard preprocedure assessment forms are filled out, including any medications the patient takes with the times of the last doses noted. The family is shown to the radiology waiting area, and the immediate pre-operative assessment begins.
Outpatients who report for an interventional radiologic procedure who have not had a blood test within the past two weeks should first have lab work done. As mentioned earlier, the basic requirements for an invasive procedure are a PT, INR, PTT, and platelet count. Other tests pertinent to the individual patient's status may have been ordered. The blood is labeled for immediate processing, and the results should be sent to the admitting area and the radiology department or compiled in the computer where they may be easily accessed. From there, the patient is escorted to the area that functions as a short-stay admissions department.
A brief history is obtained, and baseline vital signs are taken and recorded. An intravenous line is established, and a keep-vein-open unit of IV fluid is started according to pre-established standing orders. When it is time for the scheduled procedure, the patient is brought to the holding area of the radiology department. The protocol that is used to check patients into the surgical suite is followed, and the patient is brought to the designated interventional room. By this time, just as in an operating room, sterilized equipment and instruments have been opened and left covered in preparation of the procedure. The patient is then positioned for the procedure. In the area where the puncture will be made, the skin should be disinfected and covered with sterile sheets. A local anesthetic can be administered after a second disinfection of the area.
To summarize, certain steps should be followed before administration of any sedation begins. All patients should be seen and evaluated by a physician involved in the procedure. An informed consent form should also have been obtained at that time. The chart should be reviewed, along with any medications or treatments given to the patient within the last few hours. Electrocardiograms (EKGs), current laboratory data, and consults or pertinent notes should be included. Related radiologic films should be present in the room for evaluation and comparison during the case.
The physician and nurse should assess baseline vital signs, history of drug allergies, neurologic status, anxiety level, discomfort, and any prior medications taken since the patient's arrival in the hospital. If the patient is a hospital inpatient, all recent data in the chart should be reviewed. If the patient is a diabetic and has been NPO, the latest insulin injection or oral diabetic agent and most recent blood sugar should be carefully evaluated. If the patient has received an insulin injection, a dextrose intravenous solution may be started. The IV line should be checked for patency, flow, and any signs of infiltration or phlebitis. If the line must be restarted, the radiology nurse does so before continuing with any further procedures.
Certain invasive procedures, such as biliary or kidney drainages, require that the patient be pre-medicated with intravenous antibiotics. If the medication has not been given, the radiology nurse should administer a dose. A special procedures record or surgical report is kept in the room for documentation of all events and medications.
Unless the patient is not a candidate, IV moderate sedation is used in almost all cases. Children and patients who are not cooperative may require general anesthesia or very heavy sedation to keep them comfortable and quiet during the procedure. Circumstances such as these sometimes require the services of an anesthesia provider.
Because moderate sedation (formerly called conscious sedation) is used so commonly in interventional radiology, it will be discussed briefly in this section. In 2001, the Joint Commission developed a new definition of moderate sedation that is widely accepted and used. Moderate sedation is defined as a minimally depressed level of consciousness, during which the patient retains the ability to maintain a continuously patent airway and respond appropriately to physical stimulation or verbal commands [28,29]. The objectives of moderate sedation are mood alteration, maintenance of consciousness and cooperation, elevation of the pain threshold with minimal changes in vital signs, partial amnesia, and a prompt, safe return to activities of daily living.
The importance of a detailed preprocedure physical assessment has already been established because there are instances when certain patients are not proper candidates for administration of these types of agents. The Joint Commission requires a presedation assessment of each individual prior to beginning moderate sedation [30]. During the procedure, the staff should constantly be alert to any changes in the patient's condition and be prepared to assist in managing any complications that may develop [28].
Policies concerning the responsibilities in the administration of moderate sedation vary by state, by institution, and by recommendations from national accrediting agencies such as the Joint Commission. All members of the team providing moderate sedation should be fully aware of policies that are relevant to their job description. Written policies should address patient selection, monitoring responsibilities, documentation, and minimum time spans for recording vital signs, oxygen saturation, and cardiac rhythms.
In addition, it should be clear which medications the radiology nurse may be allowed to administer and which should be given by a physician. Registered nurses who administer moderate sedation should receive special education and training relevant to its use, and they should be certified in critical care, CPR, and IV therapy. Competency examinations should be given yearly or as suggested by established criteria. Every clinician providing sedation should recognize the patients who are at risk and, if extenuating circumstances arise, should be comfortable to say that he/she is not adequately trained in providing sedation to this particular patient. There should be no pressure to provide sedation when suitability criteria are not met.
The American Society of Anesthesiologists has developed a Physical Status Classification System to determine risk for complications among patients undergoing anesthesia (Table 4). This scale is frequently used in the moderate sedation setting and easily performed on all patients. Patients categorized as Class ASA I or ASA II are considered good candidates for moderate sedation procedure; those in Class ASA III or higher carry greater risks.
AMERICAN SOCIETY OF ANESTHESIOLOGISTS PHYSICAL STATUS CLASSIFICATION SYSTEM
| Physical Status | Definition |
|---|---|
| ASA I | A normal healthy patient with no systemic disease |
| ASA II | A patient with mild-to-moderate systemic disease |
| ASA III | A patient with severe systemic disease |
| ASA IV | A patient with severe systemic disease that is a constant threat to life |
| ASA V | A moribund patient who is not expected to survive without surgical intervention |
| ASA VI | A declared brain-dead patient whose organs are being removed for donor purposes |
The surgical or special procedures record should specify the different monitoring devices used during moderate sedation administration and the doses and exact times of all supplemental medications given. Oxygen therapy should also be recorded. Documentation should reflect the postprocedure care given as well as the particular discharge criteria used. One of the most commonly used discharge scoring systems is the Modified Aldrete Score (Table 5). A score of 18 or higher indicates a patient's readiness for discharge [32,33].
MODIFIED ALDRETE SCORE
| Domain | Criteria | Score |
|---|---|---|
| Activity | Able to move 4 extremities voluntarily on command | 2 |
| Able to move 2 extremities voluntarily on command | 1 | |
| Able to move no extremities voluntarily on command | 0 | |
| Respiration | Able to breathe deeply and cough freely | 2 |
| Dyspnea or limited breathing | 1 | |
| Apneic | 0 | |
| Circulation | BP±20% of pre-anesthetic level | 2 |
| BP±22%–49% of pre-anesthetic level | 1 | |
| BP±50% of pre-anesthetic level | 0 | |
| Consciousness | Fully awake | 2 |
| Arousable on calling | 1 | |
| Not responding | 0 | |
| Oxygen saturation | Able to maintain oxygen saturation >90% on room air | 2 |
| Needs oxygen inhalation to maintain O2 saturation >90% | 1 | |
| O2 saturation <90% even on oxygen supplement | 0 | |
| Dressing | Dry | 2 |
| Wet, but stationary | 1 | |
| Wet, but growing | 0 | |
| Pain | Pain free | 2 |
| Mild pain | 1 | |
| Pain requiring parenteral medications | 0 | |
| Ambulation | Able to stand up and walk straight | 2 |
| Vertigo when erect | 1 | |
| Dizziness when supine | 0 | |
| Fasting-feeding | Able to drink fluids | 2 |
| Nauseated | 1 | |
| Nausea and vomiting | 0 | |
| Urine output | Has voided | 2 |
| Unable to void, but comfortable | 1 | |
| Unable to void, but uncomfortable | 0 |
The interventional radiology rooms should have immediate access to emergency equipment, with airways, suction setups, and first-line drugs present. A fully equipped crash cart should be immediately available. Before any medication administration is started, the Joint Commission requires that heart rate and oxygenation be continuously monitored by pulse oximetry in all patients undergoing moderate sedation [29]. Baseline readings are taken and recorded. If the patient is to receive supplemental oxygen therapy, a pulse oximetry reading on room air should be documented. After oxygen therapy is initiated, another pulse oximetry reading should be obtained.
Radiologists use local or regional anesthetics for local pain control, usually concurrently with IV moderate sedation. Although policies vary, many states require that the physician administer the first dose, with supplemental doses given by the nurse as long as the physician remains physically present in the room. Intravenous moderate sedation agents have a rapid onset and most often are administered in small dose increments. They are broken down into two categories: opioids and sedatives.
The most commonly used opioid analgesics include meperidine, morphine, fentanyl, and remifentanil. Under their effect, the patient may be aware of painful stimuli, but the stimuli may be perceived as distant and not acutely painful. Opioids relieve dull, continuous pain better than sharp and intermittent pain, so local anesthesia is still necessary for patients undergoing procedures such as these. Fentanyl is given in doses measured in micrograms because it is 100 times more potent than morphine and should be titrated according to the response of the patient. While opioids can also provide a degree of sedation, the sedative drugs have no effect on pain. They are given to reduce anxiety and also to provide some degree of short-term amnesia [34,35].
Diazepam, midazolam, and lorazepam are the sedatives most commonly used in moderate sedation. Midazolam works a bit faster than diazepam and does not usually cause the transient irritation to the vein that may be seen when intravenous diazepam is given. Midazolam is three to four times more potent than diazepam and has a shorter action duration, so it is the drug of choice at many facilities.
Respiratory depression is the main adverse effect of IV moderate sedation. Because of this, it is advisable to administer smaller doses, making certain that the total effect of the drug has been fully evaluated before any further doses are given. In addition to the required emergency equipment, it is prudent to have reversal agents directly on hand. Naloxone is a narcotic antagonist and is the drug of choice to counter effects of the opioids. Flumazenil partially or completely reverses the sedative effects of the benzodiazepines (midazolam and diazepam) [20]. Because several doses of both these reversal agents may be needed, careful titrating is necessary. It is advisable to have dosage charts available for emergency use, so valuable time is not wasted trying to calculate how much of which drug should be given.
In addition to keeping advanced life support equipment and emergency equipment on hand, the staff should remember to employ basic measures used in case of respiratory depression and hypotension. Trendelenburg positioning and proper positioning of the head may be all that is required to help restore blood pressure and normal airway status.
After the radiologic procedure is completed, patients should be observed very carefully until they are fully awake, alert, and stable. Discharge back to the same day or short-stay area should be carried out only after the patient meets written criteria. Prolonged sedation may dictate that the patient be observed in the postanesthesia care unit (PACU) or recovery room for a longer period of time.
The number and extent of interventional procedures is increasing at a rapid rate. The SIR identifies some of the most commonly performed procedures [36]:
Biopsy
Drainage
Angiography
Angioplasty
Central venous access
Embolization
Chemoembolization
Stenting and grafting
Fallopian tube catheterization
Hemodialysis access maintenance
Radiofrequency ablation
Thrombolysis
Transjugular intrahepatic portosystemic shunt (TIPS)
Uterine fibroid embolization
Some of these procedures will be discussed in detail in the following sections. The reader is referred to current literature for a continual, up-to-date analysis of available procedures.
Biopsies have been performed at the bedside for many years. With the aid of procaine and a sampling needle, the physician was able to "blindly" take a sample of tissue, such as the liver, that was sent to the laboratory for analysis. It was not until cross-sectional imaging became available in the 1970s that the diagnostic potential of needle biopsy was fully appreciated. Today, interventional radiology percutaneous biopsies can diagnose primary or metastatic malignancy, tumor recurrence, and staging, infection, and other disorders [37].
The art of CT, MRI, ultrasound, or fluoroscopy now allows the great majority of tissue abnormalities to be safely sampled [37]. The success and risk of needle biopsy procedures depend on a number of factors. The patient should be reasonably capable of cooperating during the procedure; for example, the patient should be able to remain totally still and not breathe during needle placement. The area being sampled should be readily identifiable on the image, and the clinician should be skilled at the procedure, able to avoid major blood vessels, the bowel, and other potentially hazardous areas.
To make an accurate diagnosis, the specimen should be handled properly. It should be taken directly to the cytopathologist, although more often the pathologist, or a staff member, comes directly into the interventional radiology room to care for the specimens. According to the working diagnosis, care should be taken to ensure that the tissue is sent for culture and appropriate staining. Having the pathologist present is immensely helpful to determine what types of additional studies might be indicated. The radiologist usually obtains several tissue samples as multiple specimens increase accuracy.
Organ biopsy may be performed under ultrasound guidance, which has been shown to produce good results in some small abdominal and pleural lesions. In some cases, however, it may be difficult to visualize the tip of the biopsy needle, but this modality is preferred by some interventional radiologists. Fluoroscopy with C-arm may also be used for biopsy procedures. This technique is capable of helping the physician determine accurate needle placement. CT is used when biopsying deep lesions and can guide the operator past large blood vessels or intestines. CT scanning provides the most anatomic detail and can be used to plot a safe pathway to the lesion. The new scanning modalities and sampling needles have made the procedure faster and more precise.
Most often, the patient who presents for biopsy has already undergone a diagnostic CT scan, ultrasound, or MRI. The films are ready, and the desired and detailed approach to the procedure has already been determined. If there is any uncertainty at the beginning of the case, the scan may be repeated with or without intravenous contrast agents. Oral contrast material, which is given for CT scans of the digestive system, may also be indicated at that time if there is any question concerning the area involved.
Biopsies involving a specific area or small lesion take somewhat longer and are a bit more involved than those involving a random sample of a tissue. Examples of general organ biopsies include a liver biopsy to diagnose or stage hepatitis C or a kidney biopsy to determine amyloidosis.
Tissue sampling techniques vary, but general principles remain constant. There are many different versions of sampling needles, but all should be able to permit recovery of enough material to allow both cytologic and histologic studies. The needles should be sharp enough to enter small, hard lesions without pushing them aside. The choice depends upon the kind of imaging modality used, the type and location of the lesion, and perhaps most importantly, the preference of the clinician. Biopsies are performed in short steps, no matter which type of guidance has been selected. In all cases, the skin is numbed with an anesthetic, such as lidocaine 1%, followed by infiltration of the deeper tissue. A small puncture with a scalpel may be made to aid the passage of the needle, which is inserted and followed by imaging to check for placement. Several sequential images assure that the needle is in place in the desired target tissue.
The American College of Radiology states that definitive diagnosis of a mediastinal mass by biopsy is vital in that it may significantly change the treatment options or may preclude the need for exploratory surgery. Image-guided biopsies of mediastinal masses are almost always performed using CT guidance.
(https://acsearch.acr.org/docs/69343/Narrative Last Accessed: June 1, 2022)Level of Evidence: Expert Opinion/Consensus Statement
Improved imaging capabilities and biopsy techniques have made it possible to obtain tissue samples from most lung lesions, including some that measure less than 1 centimeter in diameter. Bronchoscopy is performed for central endobronchial lesions, but percutaneous needles can safely approach most other thoracic masses. Needle biopsy of the thorax is performed when there is a reasonable suspicion of malignancy, to confirm what appears to be a benign lesion, to obtain samples of what seems to be infectious material, and to aid in staging patients with neoplastic extension to the hilum, mediastinum, or chest wall. False negative results have been reported, but taking multiple samples from different parts of the lesion may reduce these numbers. Depending on many factors, these false negatives may be followed by a repeat needle biopsy, open lung biopsy, or watchful waiting with regular, periodic chest x-rays [38].
How the patient is positioned during lung biopsy depends on the location of the lesion and the path the radiologist uses to reach it. The patient may be positioned on his or her back, with the head elevated slightly and arms supported above the head, or prone with the head turned to the side and the arms stretched upwards. Patients are made as comfortable as possible during the procedure and soft restraints or armbands are applied to provide comfortable positioning of the extremities.
The most common complications from thoracic biopsy are collapsed lung (pneumothorax) and minor bleeding leading to coughing blood (hemoptysis). It is not uncommon for patients to cough up bright red blood for several hours after their procedure, and they should be warned that this may occur. Hemoptysis usually subsides spontaneously. A chest x-ray is almost always performed within 15 minutes after biopsy of the thorax to be sure that there is no pneumothorax. Some studies have found an overall frequency of pneumothorax of between 9% and 54% (with an average of around 20%), but many of these are small areas and require no treatment [39]. The single most important factor contributing to pneumothorax does not appear to be needle size, but rather the presence of chronic obstructive pulmonary disease (COPD), small lesion size, a long needle path, and repeated pleural puncture [39].
Most radiologists believe that treatment of a postbiopsy pneumothorax rarely requires a large chest tube but can easily be treated initially by the radiology department. A small (size 6 to 9 French) trocar catheter is inserted into the pleural cavity through the anterior second or third intercostal space in the midclavicular line and is connected to a one-way Heimlich valve. Usually the air leak will seal within 12 to 48 hours and does not require connection to suction. The patient most often will be admitted to the hospital, but in select cases reliable outpatients will be allowed to go home with the tube in place and return the following day for re-evaluation.
Transcutaneous liver biopsy is performed to make a diagnosis of tumor as well as to establish the cause of a disease process in that organ. Patients are routinely referred for a definitive diagnosis of hepatitis (most often hepatitis C). In cases without a particular area of suspicion, any segment of hepatic tissue may be sampled. This procedure was once known as the bedside biopsy. Due to the large size of the organ, there is usually no difficulty obtaining a sample under radiologic guidance. Some gastroenterologists may still perform liver biopsies at the bedside, but an increasing number prefer it to be performed in the CT or ultrasound departments. The liver biopsy is performed with greater ease and safety this way, especially with obese patients.
When a liver biopsy is performed to sample a specific area of tissue, the ultrasound or CT guides the radiologist to the exact position of the lesion. It is often possible to differentiate a hemangioma or benign vascular liver tumor from other masses by certain noninvasive procedures such as a blood flow study combined with a tomographic liver scan performed in the nuclear medicine division or by other modalities. For obvious reasons, lesions comprised of blood vessels should not be biopsied, but occasionally it is not possible to clearly differentiate a hemangioma from a malignant tumor. In cases where there may be some uncertainty, biopsies may be warranted although extra care should be taken and a smaller biopsy needle used.
At times, transjugular liver biopsy may be performed for conditions such as massive ascites and coagulopathies. With this method, the liver is not approached through the abdominal wall, but rather via the jugular vein. All instrumentation is performed through the venous system, with long wires and sampling forceps threaded down through the vascular system into the liver.
The medical oncologist should ascertain the primary source of cancer before considering chemotherapy or any other treatment. Liver biopsy can be used to differentiate between a primary liver cancer and a metastatic tumor. There are times when masses that appear to be some type of metastasis result in a totally different and welcome diagnosis. Liver biopsy often provides this information.
Because the liver is a highly vascular organ, as are certain types of metastatic lesions, bleeding is the most likely complication of liver biopsy. Many patients with liver disease or cirrhosis have alterations in their clotting mechanisms, which puts them at increased risk for bleeding. When cutting needles enter these areas, there is always a potential for hemorrhage.
Immediately after liver biopsy, many patients complain of pain in their right shoulder and believe this to be muscular due to their position on the scanning table (arms over their heads.) Actually, the pain is usually due to a few drops of blood that have dripped onto the diaphragm, stimulating the phrenic nerve, which becomes a trigger for referred pain. Most patients find relief with acetaminophen, and the discomfort usually subsides rapidly. More serious bleeding or bile leaks are two of the more dangerous complications from percutaneous liver biopsy. In cases like these, patients may exhibit classic signs of acute abdomen, hypovolemia, and sepsis. Although uncommon, staff members should be aware of the potential for these complications [40,41,42].
Kidney biopsies are extremely helpful to pinpoint an exact diagnosis in a patient experiencing kidney disease. Lupus-like syndromes and types of tubular interstitial disorders may be diagnosed accurately by examination of kidney tissue. Cellular changes, atrophy, and neutrophil infiltration all may be seen by the pathologist, and these factors aid the nephrologist in treatment planning and prognosis. Renal biopsies are also performed to aid in tracking rejection after a kidney transplant. Some smaller hospitals send their renal specimens out to a laboratory that specializes in analysis of renal tissue because the care and examination of renal specimens are quite involved. The kidney biopsy itself, however, may be performed in general interventional radiology departments.
Patients are positioned prone for kidney biopsies. Specimens are collected by means of long sampling needles. The procedure is usually safe, but some caveats apply, as in sampling for lupus. Sampling error can occur, and the experience of pathologists in reading lupus nephritis biopsy specimens varies considerably [43,44]. Many referring physicians prefer to admit their patients overnight, just to be sure that any excessive bleeding may be noted.
Long needles may also reach tumors of the adrenal gland. Due to the adrenal's location on the superior pole of the kidney, the technique for positioning is almost exactly the same. The physician isolates the solid tumor by CT scan or ultrasound guidance and obtains a sample for analysis. Caution should be practiced with adrenal biopsies because the possibility always exists that the mass is a pheochromocytoma. This tumor consists of cells that secrete adrenaline and other catecholamines and can cause paroxysms of hypertension, tachycardia, headache, nausea, diaphoresis, and a multitude of similar symptoms [45]. Care is always taken not to stimulate a pheochromocytoma, so piercing it with a needle should be avoided.
Pancreatic carcinomas may be extremely difficult to diagnose; however, needle biopsy of the pancreas is a very helpful technique. There are times when fibrotic tissue forms around the tumor area that will result in a false negative if this is the site that is sampled. Pancreatitis, a serious complication after pancreatic biopsy, should be looked for after the tissue is needled. This occurs less often in larger lesions that have more fibrotic areas. Most cases of pancreatitis, if they do occur, will subside after a few days. As with liver biopsy, patients are positioned supine for pancreatic biopsy with their arms supported back and over their heads. Ultrasound or CT are the usual imaging modalities and are necessary for accurate sampling.
Biopsies of the spine, ribs, pelvis, and other bones may be performed under CT or fluoroscopic guidance. Fluoroscopy offers the advantage of real-time imaging, which may be useful for difficult needle guidance; however, CT is the preferred modality for instances when there are many soft tissue structures that should be avoided, as fluoroscopy is unable to visualize soft tissues. Therefore, when fluoroscopy is used, a radiologist should have ample experience and knowledge of anatomy.
Patients who undergo bone biopsy may feel a bit more discomfort than those having soft tissue biopsies. The pain is usually experienced as the needle penetrates the periosteum. Many bone lesions are lytic and softer; in these cases standard biopsy needles may be used. Specialized bone needles are often used, frequently retrieving blood as well as tissue. The blood should be sent to the laboratory along with the tissue as malignant cells may be isolated from the blood clot.
Patients are positioned according to the area being biopsied. Disk space biopsies may also be performed after consultation between the radiologist and orthopedist or neurosurgeon. Patients with disc space disease usually have fever, pain, and elevated white blood counts and erythrocyte sedimentation rates. The generous use of opioids and sedatives makes bone biopsies much easier for patients who undergo these procedures [46].
Percutaneous biopsy of soft tissue masses and enlarged lymph nodes in the abdomen or pelvis may confirm the suspected diagnosis of Hodgkin and other lymphomas, sarcomas, and other malignant tumors. Most often, diagnoses are already fairly certain, but these procedures provide the oncologist vital information used to plan treatment, which may be palliative or curative.
Abdominal mass biopsy is performed with the patient supine, as for liver and pancreatic biopsies. Pelvic masses may be sampled with the patient in the prone position. The needle may be inserted at the top of the buttock and threaded deep into the pelvis. The needle is most often moved along with the help of the CT imaging and samples of the tumor are removed in this way for analysis. While there is a slight risk of bleeding or peritonitis, the benefit of securing a definite diagnosis almost always outweighs it. There are usually no sequelae even if a part of the bowel is inadvertently punctured. Needles that are 20 gauge or smaller usually do no harm, and the area traversed is rarely damaged.
The development of cross-sectional imaging has made it possible to perform drainages of deep body cavities without subjecting the patient to open surgery. Abdominal, pelvic, or other soft tissue fluid collections and abscesses may be safely approached and drained by percutaneous catheters. Depending on the diagnosis and site of fluid collection, the interventional radiologist most often can predict whether a drainage catheter is going to be left in place or if the entire area is going to be drained and the catheter removed. Percutaneous drainages are most often performed under CT scan or ultrasound guidance; fluoroscopy is used less frequently. Drainages are often performed simply for diagnostic aspiration. Specimens are withdrawn and sent to the laboratory for culture and sensitivity, cytology, and multiple chemistry analyses. Tests such as these can aid in making the diagnosis of abscess, hematoma, biloma, and malignancy.
There are some instances in which fluid may be obtained as a bedside procedure, without the need for imaging techniques. Bedside paracentesis and thoracentesis are relatively common events in all hospitals, but there are many situations where these routine procedures are not possible. For example, obese patients benefit from radiologic guidance because the patient's abdominal pannus often presents a difficult or even impossible mechanical obstruction to the sampling needle. Large tumor masses may also pose problems for the operator. It may be unsafe to attempt penetration of the abdominal cavity with areas of vascular tissue situated in the space to be entered. Care always should be taken to avoid bowel, spleen, and major blood vessels. Puncturing the diaphragm may lead to serious problems for the patient, so the clinician should be aware of the individual patient's anatomy. As a result, it has become increasingly common for physicians to ask the interventional radiologist to perform abdominal fluid sampling and drainage of ascites under the guidance of the ultrasound or CT scan.
While it is often possible to drain a large area of abdominal fluid with one drainage catheter or needle, the CT or ultrasound image may point to several multilocular sites, which would require more than one puncture. Sometimes in cases such as these, especially when abdominal abscesses are present, the recommendation is to take the patient to the operating room and perform a surgical incision and drainage with abdominal irrigation. The same is true for abscesses that have formed around infected surgical grafts. It is common, however, for the radiologist to drain two areas of fluid collection at the same time when the pockets of material are not connected and massive contamination is not suspected.
There are times when the fluid is found to be so viscous that draining presents a problem. While it is possible to irrigate through the catheters or instill medication to make the fluid less viscid, the overall results in these cases are usually less than optimal. All drainage procedures involve the same basic preparations as are required for biopsies. Histories, clinical assessments, and laboratory and chart reviews are standard. Anything pertinent to the case is evaluated and discussed before the procedure starts. Patients are either kept fasting or allowed only clear liquids. The skin is prepped and draped, and local and deep infiltration is performed with 1% lidocaine; moderate sedation is administered as necessary [47].
Abdominal paracentesis is perhaps the most straightforward drainage procedure for the interventional radiologist. The area of ascites is clearly documented on sonogram or CT scan, and the physician can usually tell if there is a large quantity of fluid present that should be removed. The patient is positioned supine on the scanning table with his or her arms supported above the head. After the initial puncture and release of fluid, specimens are usually collected and sent for analysis. If the goal is simply diagnostic aspiration, the procedure may end there by withdrawing the needle and covering the site with an adhesive bandage or small gauze dressing. For therapeutic drainage procedures, however, the radiologist attaches drainage tubing, then attaches it to a vacuum bottle. As each bottle fills, the tubing is clamped, removed from the bottle and inserted into the next. As the clamp is opened, the next bottle fills.
Many liters of fluid may be removed this way, although care should be taken to ensure that the sudden release of pressure in the abdomen does not cause any detrimental hemodynamic effects to the patient. At times, the radiologist may stop the procedure after a certain volume has been withdrawn to prevent any such problems. If a very large amount of abdominal fluid is drained, the radiologist or patient's referring physician may order some intravenous volume replacement with albumin or other similar solution. An immediate postprocedure image will show the size of any remaining ascitic collection.
Paracentesis for recurrent ascites may require repetition on a regular basis. Therapeutic paracentesis is indicated for patients with tense ascites resulting in respiratory difficulty, pain, or even compromised renal function. There may be leakage of ascitic fluid at the site of the needle puncture, so the dressing should be changed as needed. Newer techniques may permit a surgeon to implant a drainable abdominal catheter, such as a Tenckhoff catheter, to allow intermittent drainage of the ascitic fluid without subjecting patients to repeated punctures [48].
Although serial paracentesis can reduce symptoms in some patients, indwelling catheters provide an alternative approach that allows patients to manage their symptoms at home. One literature review identified 14 studies that included 957 patients with indwelling catheter placement for chronic ascites (687 with malignancy and 270 with cirrhosis) [49]. Catheter dysfunction was the most common complication reported (5.7%). Infection rates were 5.4% for patients with malignancy and 12.2% for patients with nonmalignant ascites. The risk of infection increased significantly with devices left in place for more than 12 weeks. Symptom improvement was reported in all 14 studies [49].
Untreated intra-abdominal abscesses have a very high degree of mortality. Abscesses may form from various sources, such as complications of acute appendicitis, severe diverticulitis, or a perforated viscus. Abdominal abscesses may also form after disruption in a suture line or from conditions such as Crohn disease. The mass may cause partial or complete bowel obstruction.
Before draining a fluid collection, radiologists usually insert an 18- or 20-gauge needle to aspirate the first sample of liquid. Following this, the drainage fluid is collected, properly labeled, and sent to the laboratory for complete analysis. While most patients who have a suspected intra-abdominal abscess are already receiving intravenous antibiotics, an initial preprocedure dose may be administered for those who are not. Some patients with therapeutic blood levels of antibiotics still develop signs of sepsis after their abscess is punctured and the contents manipulated. These patients require excellent medical and nursing care after the procedure to assure that the infection is controlled [50,51,52].
Two techniques of abdominal drainage may be used. In the first, a standard angiographic needle is inserted, followed by a guide wire, dilator, and drainage catheter. Certain tracts should be dilated to accommodate the sump catheters. In the second technique, the catheter enters over a metal cannula that has a sharp stylet. The stylet is removed once the tip is in the fluid collection, a guide wire follows, and the drainage catheter is inserted over the wire.
Depending on the consistency and amount of the abscess fluid, various types of collection equipment may be used. Catheters with side ports and different size lumens are used to drain more viscous collections, whereas thinner fluid may empty satisfactorily by means of standard angiographic, biliary, or nephrostomy catheters. These drainage catheters are usually attached to some sort of battery powered collection device. There are instances, however, when the radiologist is certain that the entire abscess cavity has been drained. In these cases, the catheter is withdrawn and the site covered with a dry, sterile dressing. Imaging is performed immediately before catheter removal to document emptying of the abscess cavity.
Any drainage catheters left in place are safely secured and dressed by the radiology nurse or interventional radiology technologist. If two areas have been drained and have separate catheters in place, the sites and drainage equipment should be clearly labeled so they may be properly differentiated. Orders are written to specify the care of the catheter and request careful measurement and emptying of the drainage chambers. Occasionally, a very reliable and stable patient may be sent home with the catheter in place. In this case he or she is given detailed instructions regarding the care of the catheter and related equipment as well as names and telephone numbers to call if any questions or problems arise. The patient is told when to return for possible catheter removal. Any radiologically placed drainage catheters should be removed by the interventional radiologist and not the patient's referring physician.
Drainage catheter removal is based on several principles. The tube should come out when there is insignificant drainage or cessation of drainage and radiologic imaging shows proper catheter position. Removal can also take place when the patient demonstrates clinical improvement and the signs and symptoms of infection have significantly diminished. Also, if the CT scan documents the absence of residual abscess and the collection does not reaccumulate when the tube is clamped, it is time for it to be removed [50,51].
The decision to do a radiologically guided transcutaneous thoracic drainage depends on many factors, not the least of which is the preference of the pulmonologist or thoracic surgeon. Thoracenteses are commonly performed at the bedside with the clinician simply using the chest x-ray and his or her own clinical assessment of the patient for position location. At times, however, it is felt to be more prudent to use radiologic guidance [53]. In ultrasound, patients undergoing thoracentesis are positioned sitting up on the side of the stretcher; on the CT table they are either prone or supine.
The safe and effective performance of thoracentesis was the focus of one systematic literature review [53]. Sixty relevant studies were identified that included preprocedural topics such as physician training and skill maintenance (e.g., simulation with direct observation). Intraprocedurally, ultrasound use was associated with lower risk of pneumothorax. Pleural manometry helped identify a nonexpanding lung and reduce the risk of re-expansion pulmonary edema. Postprocedurally, the studies indicated that routine chest x-ray was unwarranted because bedside ultrasound was able to identify pneumothorax [53].
Thoracic empyema, once always drained in the operating room along with a chest decortication, now may be performed in the radiology department under CT assistance. The cross-sectional CT images allow the radiologist to have a detailed look at the precise location of the fluid collection. An already very ill and compromised patient may be spared a more invasive procedure in which general anesthesia is required. When the pleural space is drained, the indwelling catheter is most often connected to a water seal set-up, such as the Thora-Seal or Pleura vac type. This is necessary to ensure that no air enters the pleural space, as this would inhibit full expansion of the lungs.
Although video thoracoscopies have replaced many standard thoracotomies, patients still require deeper anesthesia than is given in simple drainage procedures, so radiologic guided chest drainages have a very important function [54].
Pelvic abscesses usually are complications of acute appendicitis, pelvic inflammatory disease (PID), or colonic diverticulitis. Some signs and symptoms are leukocytosis, fever, and lower abdominal pain, along with diarrhea or urinary symptoms. As with other abscesses, treatment includes antibiotic therapy and drainage of the purulent material.
Tubes that drain air usually are positioned in the most superior aspect of the involved region. With fluid, the opposite is true because gravity is used to aid in the drainage. Because a drain is best placed in the most dependent portion of an abscess, it may be necessary to reach a pelvic abscess through the gluteal muscle. The gluteal muscle is a relatively large and heavy muscle, so a stiffening cannula may be required. The procedure may be quite uncomfortable for the patient, and liberal use of opioids along with sedatives may be indicated.
Pelvic abscesses are most often drained with the patient prone on the imaging table. Catheters are hooked to a suction device with special care being taken in proper dressing of the area. It is important that the patient's comfort be considered when taping the tubing in place, especially if a three-way stopcock has been attached for irrigation purposes. It may be uncomfortable for the patient to lie supine in bed with certain setups in place; therefore, the radiology nurse or special procedures technologist should pad the area considerably with gauze and ensure that the catheter will not become kinked [51].
A surprising percentage of the population has undetected visceral cysts, many of which are located in the kidney, liver, and pancreas. Although most cysts go unnoticed until discovered accidentally during an unrelated imaging procedure, some grow large enough to cause symptoms. An interventional procedure may be recommended when symptoms arise or when a particular cyst appears suspicious.
Hepatic cysts, unless due to infections, very large, or multiple, usually have no real clinical significance and are found mainly on CT scans or other imaging procedures. Cysts in kidneys may be of several types and may vary in size from less than 1 centimeter to more than 10 centimeters in diameter. A person may have multiple cysts, such as in polycystic kidney disease, or isolated cysts arising from the renal cortex or medulla. Some cysts are of hereditary origin while others have an inflammatory or neoplastic etiology.
Renal cysts cause symptoms when they grow large enough to exert pressure on the surrounding tissue and produce a mechanical obstruction to normal renal function. In addition, the pressure from a huge renal cyst could cause extreme displacement of the kidney itself, a situation that is obvious on intravenous pyelogram (IVP) or abdominal CT scan. Renal cysts can be drained in the CT or ultrasound departments by means of a long needle and drainage catheter. The patient is positioned prone on the interventional table and intravenous sedation is usually given along with local anesthetic. Renal cyst drainage is generally a same-day procedure, with the patient able to go home even after the aspiration of more than two liters of fluid. In cases like these, immediate follow-up films usually show that the kidney has returned to its normal position. Cystic fluid is usually straw colored and clear. While samples of renal cystic fluid are generally sent for lab studies, the overwhelming majority are found to be sterile and benign. As with any cyst that is not totally removed, there is always a potential for recurrence.
Most pancreatic cystic lesions are inflammatory pseudocysts, but 10% of pancreatic cysts are ductal neoplasms, some of which are pancreatic carcinoma. Because of the potential for misdiagnosis of types of pancreatic cystic tumors, precise laboratory examination is essential. Aspiration of pancreatic cystic fluid may yield less than one to several hundred cubic centimeters of fluid and is most often performed with the patient supine on the CT table. While many highly specialized exams may be performed to diagnose the exact type of pancreatic lesion, errors may occur as experience with cystic fluid analysis is still somewhat limited [55,56]. Measurement of glucose in cystic fluid has emerged as a promising diagnostic technique [57,58]. Studies of tumor biomarkers (e.g., proteomic cyst fluid mucin, cell-free DNA, cell-free RNA, circulating tumor cells, circulating tumor proteins, extracellular vesicles) may lead to the development of more effective methods for the early detection and diagnosis of pancreatic cancer [59,60,61,62].
The benefits of draining a questionable cyst should be weighed against the risks, including complications from the procedure itself and the risk of disseminating a malignant tumor by spilling the cyst contents into the peritoneum. Studies urge caution before attempting to drain what almost certainly appears to be a pseudocyst of the pancreas because errors in diagnosis may come from making interpretations from technically suboptimal images [63]. Studies suggest that endoscopic- and image-guided drainage may be feasible, effective, and safe [64,65].
The ability to perform percutaneous nephrostomy (PCN) has led to an entirely new approach to the treatment of urologic disease. First used solely for the decompression of obstructed upper urinary tracts, it now can be used to obviate open surgery, which is usually accompanied by protracted recovery periods. Even the advent of extracorporeal shock-wave lithotripsy (ESWL) has not eliminated the need for the percutaneous approach to the collecting system of the urinary tract for some patients with kidney stones [66,67,68].
PCN provides a less invasive means to drain the renal collecting system in cases where obstruction of the kidney and ureter has resulted in hydronephrosis. Most often used for patients with kidney stones or bladder or pelvic tumor obstructions, PCN may be used to divert urine from the renal collecting system to allow leaks and fistulas to heal [67]. The procedure is often performed after attempts at placing a ureteral stent through retrograde cystoscopy have proven unsuccessful. Hence, it is vital that the urologist and radiologist consult and work as a team. In cases of ureteral obstruction, radiographic images often show an obstructive hydronephrosis. Providing drainage for that kidney is an urgent necessity, and PCN provides an exact method of accomplishing this task.
The access provided by nephrostomy allows ureteral strictures to be dilated and stents to be placed as needed. The stent provides a means to hold open an area that is contracted or constricted. PCN provides a means by which infected urine may drain and the reflux and damage caused by the obstruction may be relieved. Before performing PCN, the patient will have undergone several procedures to obtain the most information possible. Ultrasound of the kidney and an IVP will most likely have been performed, possibly along with nuclear medicine and CT scans [67].
It is sometimes difficult for the patient and family to grasp the concept of PCN, so the radiology staff, including physicians, should begin with a basic discussion of the anatomy and physiology of the genitourinary system. By explaining to patients that the kidney makes urine and that it drains down through the ureters into the bladder, they should be able to understand the importance of providing an outlet for such drainage. Patients and family should realize that PCN is not a one-step procedure that will result in an end to the problem; it is a part of the entire therapeutic intervention, which may take several days or weeks to complete.
To stress the need for teamwork between the interventional radiologist and the urologist, it should be understood that the removal of multiple stones in the renal collecting system depends on the point of entry of the nephrostomy tube. Once the kidney drainage has been established in the radiology department, the urologist is able to proceed with stone removal in the operating room via the PCN tract. In some instances, the interventional radiology team goes to the operating room and the first part of the procedure is performed on the operating table, with portable fluoroscopy as the guidance mechanism.
Patients undergoing PCN should be treated with antibiotics and should receive an intravenous dose within one hour of the procedure being initiated [67]. There is a high incidence of septic shock in patients with upper urinary tract infection, even with antibiotic prophylaxis. Because kidney stones are commonly associated with infection, premedication with antibiotic therapy is commonly used when stones are thought to be present. The most common urinary pathogens are gram-negative bacteria, thus administration of the antibiotic is continued for at least 48 hours after the procedure. Nephrostomy tube placement is most often performed with local anesthesia along with IV moderate sedation. General or epidural anesthesia is indicated only if extensive tract dilatation is planned prior to stone removal.
The approach is extremely important for PCN, and the procedure is performed under ultrasound or fluoroscopic guidance. In some cases, a small amount of intravenous iodinated contrast is administered at the start of the procedure to opacify the collecting system [67]. The patient is placed in the prone position with both arms above his or her head or one arm up and the other at the noninvolved side. The entry site is prepped and draped and infiltrated with local anesthetic. A small puncture is made with a scalpel, and a posterior lateral approach is made with a needle and directed toward a lower calyx of the kidney. If the tip of the needle has entered a dilated part of the collecting system, urine will flow back from the needle when the stylet is removed. A specimen should be collected and sent to the laboratory for microscopic and bacterial studies. Obviously, infected urine will be cloudy and turbid.
Once the proper position is established, various wires and dilators are used until a nephrostomy tube can be passed into position. The catheter is meticulously secured in place and attached to a properly labeled drainage bag [67]. It is normal for hematuria to be present after the procedure and to continue for one to two days. Explicit orders should be written in regard to tube output and maintenance.
Depending on the diagnosis, patients may be discharged within several days after undergoing PCN. Many cancer patients who have had palliative nephrostomies go home with the catheters in place and most often are seen by a visiting nurse. Flushes with 5 cc of sterile saline may be ordered to ensure free flow of urine [67]. Tube changes may be scheduled every 6 to 12 weeks or more frequently if conditions warrant. If the PCN is for decompression, the external drainage may be continued until the desired results are achieved and urine begins to flow naturally down the ureter. Nephrostomies that are performed for future stone removal may have the drainage part plugged until it is time for the procedure to be performed.
Hemorrhage is the major risk of PCN, but the risk can be reduced substantially with use of a very small needle. Nephrostomies are performed frequently in interventional radiology departments and are a major part of the treatment for patients with malignant obstructions, renal stones, and other kidney problems [67,69].
Ureteral stents are frequently inserted when there is a need to provide a means of holding open a stenosed portion of the ureter. Ischemia is the most common of many causes for these strictures and may result from a variety of reasons, including pressure necrosis from a ureteral stone, trauma, radiation therapy, surgical manipulation of the ureter, inflammatory disease, and chronic transplant rejection. All of these scenarios result in a diminished blood supply to the area and can initiate a cycle of ischemia, scarring, and greater ischemia.
Before patients are referred for PCN, they have almost always undergone prior urologic procedures whereby the urologist has attempted to open an obstructed ureter and establish free urine flow. A urologic stent is often placed during the cystoscopy to bypass the obstruction, but a nephrostomy is indicated when the kidney must be drained from above. PCNs are often followed by ureteral stent placement.
Certain areas of the ureter may be amenable to balloon dilation, but ureteral stenting often produces a more positive result. Stents of 6 to 8 French are commonly used for placement in ureters. While there are many types and styles of ureteral stents, and many new designs under evaluation, the most common is a polyurethane double pigtail device [70].
Stents are passed into the tract over a guide wire with a type of pushing catheter. When it is in the proper position, the stiffener is removed, the nephrostomy tube is replaced, and the guide wire is removed. It is often advisable to leave the draining nephrostomy catheter in place for one to two days after internal stent placement to allow draining urine to flush normal operative debris from the newly placed stent.
Nephrostograms, using a dye or contrast through the nephrostomy tube to assess the condition of the ureter and implanted stent, should be performed as a follow-up procedure. When the radiologist is confident that the stent is open and urine is flowing freely, the nephrostomy tube is usually removed. The patient is left with a functioning urinary system with a ureter that will hopefully remain open for a long time. The procedure leaves no external signs of any manipulation, except the small wound that should quickly begin to heal.
As healing occurs, the urologist may determine that it is time for the stent to be removed. Stent removal does not necessitate another PCN; it may be removed in the cystoscopy room with urologic instruments. In cases in which the stent must remain in place for longer periods of time, the urologist may be able to change it and place a new one through a retrograde cystoscopy procedure. Patients with malignant obstruction of the ureters must have their stents changed for the duration of their lives [71].
Percutaneous transhepatic cholangiogram (PTC) or transhepatic cholangiogram is used to establish drainage of the biliary system. The procedure is commonly performed in the interventional radiology area and obviates the need for open major abdominal surgery. This procedure is often palliative and is frequently performed on patients with nonresectable malignant disease but may occasionally be indicated for patients obstructed with gallstones [72]. It may be contraindicated, though, for patients with diffuse hepatic metastasis, liver failure, or a life expectancy of only days to weeks.
This procedure may also be indicated to treat strictures that cannot be reached during endoscopy and may be of benefit to provide preoperative drainage of bile in patients with severe active cholangitis. PTC may help clinicians predict which biliary tumors are considered inoperable. Many patients not able to be cured surgically may do well for comparatively long periods of time with the placement of a drainage catheter. Some patients are discharged with biliary catheters in place and are up and about rapidly. Much of the discomfort and aesthetic problems associated with severe jaundice and the pruritus it produces may disappear or be greatly diminished. PTC may also shorten the hospital stay and give the patient an improved quality of life.
The patient should be premedicated with intravenous antibiotics for at least one hour prior to the transhepatic cholangiogram. Special attention should be paid to PT, INR, and PTT results because patients with liver disease often will have abnormal coagulation studies [72]. The patient should understand the procedure and realize that he or she will likely have to wear a bag to drain bile following the PTC or transhepatic cholangiogram.
Liberal doses of sedatives and opioids are given, because transhepatic cholangiogram is an uncomfortable procedure. For the procedure, the skin and subcutaneous tissues are infiltrated with lidocaine 2% and a small nick is made with a scalpel blade. The interventional radiologist selects the level at which to place the needle between adjacent ribs, taking care not to go near the lung. The long needle is guided into the liver by fluoroscopy, and the exact position is determined by instillation of contrast material [72]. Studies have supported the use of extravascular contrast-enhanced ultrasonography as an alternative to fluoroscopy [73,74].
Once the operator is certain that the needle is positioned in a duct adequate for biliary drainage, various wires and introducers are exchanged until the proper drainage catheter is in place. Bile may be sent to the laboratory for culture and sensitivity, and the dressings and drainage bag are secured completely, keeping in mind both the safety of the catheter and the comfort of the patient.
In some cases, it is not possible to pass a tight obstruction on the first attempt [72]. It has been found that if the tract is allowed to rest, it may decompress, allowing success several days later. If a stricture due to tumor or stenosis can be opened, internal drainage of bile is made possible and the patient no longer has to wear a bile-collecting bag. The bile is able to drain directly into the duodenum. Most radiologists, however, prefer to keep the system on external drainage for the first few days even if the obstruction is passed, to assure adequate biliary decompression. After the bile is clear and debris free, the catheter may be capped and internal drainage begun. Even if the catheter is not removed, patients may live relatively normal lives.
The catheters are usually changed about every four to six weeks in simple outpatient procedures in the same radiology suite. Patients may be placed on oral antibiotics before their catheter changes, but the tube change is relatively quick and easy for the patient.
Biliary stents may be inserted, but their use is most frequently seen in palliative terminal care [75]. Some patients find the presence of a catheter protruding from their abdomens and the occasional leakage of small amounts of bile totally unacceptable; for these patients, stents are a viable option.
The use of internal biliary stents depends on the preference of the patient and the physician, as well as the expected life span of the patient. In cases of nonresectable pancreatic tumors, stents will often remain open for the patient's remaining few months. For slow-growing tumors, however, this may not be the best answer because one of the disadvantages of a biliary stent is that a completely new percutaneous procedure must be completed if the stent becomes obstructed. That means the patient must be put through another long and invasive procedure, something that may not be acceptable with terminally ill patients.
Patients who undergo PTC may be sent home after just a few days in the hospital. Their symptoms are relieved, and they look better. This is a welcome alternative to prolonged hospitalization with or without major surgery and is just one other way in which interventional radiology helps patients to have beneficial results with minimum risk [76].
Endoscopic retrograde cholangiopancreatography (ERCP) is a procedure performed by gastroenterologists or other specialists; it often takes place in the fluoroscopy room of the radiology department. ERCP will be discussed in this course only briefly because physicians, nurses, and surgical support are usually from the operating room staff. However, radiologic technologists operate the imaging equipment, and interventional radiologic technologists sometimes offer assistance with difficult procedures.
ERCP involves passing an endoscope through the mouth, as in upper gastrointestinal endoscopy. The patient is either given IV moderate sedation by the operating room team or general anesthesia by an anesthesiologist or nurse anesthetist. A catheter is passed through the opening of the ampulla of Vater and contrast material is injected to visualize the ducts. Precise biliary and pancreatic anatomy may be identified, and depending on the findings, therapeutic procedures may be performed by the gastroenterologist.
Common bile duct stones may be removed, tight sphincters may be released, and certain bile duct strictures may be drained through endoscopic placement of tubes or stents. ERCP is not performed during an acute attack of pancreatitis unless the pancreatitis persists and a stone is thought to be responsible. As with other interventional procedures, coagulation and bleeding disorders are contraindications. Hemorrhage and pancreatitis, although uncommon, are possible complications of the procedure.
In many cases, ERCP has replaced surgery for gallstone removal. It is a same day procedure, and patients are discharged several hours later with little or no restrictions. They are up and able to resume their normal activities the following day, and many patients do so free of the gallstones that troubled them in the past.
Before discussing any procedures that concern the blood vessels, it is important to begin with a brief overview of vascular interventional radiology. Angiography has long been used as the general term for the radiographic examination of the blood vessels. These studies are used to image physiologic and pathologic changes in the anatomy by injecting a contrast agent into specific portions of the vascular system. The key word here is "specific," as angiography is almost always used to examine a specific anatomical region. Almost any part of the body can be imaged during the angiographic study. The brain, heart, lungs, chest, abdomen, kidneys, arms, and legs all possess a myriad of blood vessels that are accessible by skilled interventional radiologists.
Angiography is best defined as the visualization of the internal anatomy of the heart and blood vessels after the intravascular introduction of a suitable contrast agent. Typically, the contrast medium is introduced by an intravenous or intra-arterial injection or through a catheter that is inserted into a peripheral vessel and guided to the desired target area. With exams such as CT scans and IVP, similar contrast is injected, but the agent usually goes in through a peripheral vein and enters the general circulation. Nuclear medicine blood flow studies are also usually performed with injection of a radionuclide agent through a peripheral vein.
Before the discovery of x-rays, the injection of materials into the vessels of the body was performed primarily on cadavers for academic purposes. The procedure was limited to the injection of various dyes or waxes that stained the tissues of the body and facilitated the study of human anatomy after dissection. This practice was continued after Roentgen's discovery and extended to the introduction of radiopaque materials that permitted physicians and anatomists to record the anatomy with x-rays. The use of this technique was not successfully applied to live subjects until about 1920, when a contrast agent was developed that could be safely introduced into the vascular system.
Improvements in equipment and the development of safer contrast agents fostered research in angiographic procedures. Angiography became a safe, reliable diagnostic technique. The newly developed catheterization procedure provided a springboard for the use of angiography for therapeutic purposes. Specific area visualization is accomplished by accessing a vessel with a needle that introduces a catheter, and manipulating the catheter so that it arrives at the desired location. In the early days of angiography, the vessel had to be surgically exposed to accomplish this task, but in 1953, the Seldinger technique was developed and has become the basis for modern angiography. With this method, the femoral artery is punctured over the middle of the medial third of the femoral head. The common femoral artery is only 3–5 centimeters long but is usually easily accessed.
Several therapeutic radiologic procedures may be performed at the same time as the diagnostic study, although others can be performed as follow-ups on a subsequent day. All patients undergoing angiography should be carefully prepared, just as those having any type of invasive radiologic procedure. Patients are kept fasting, except for extra water, which they are asked to drink the morning of the procedure. This liquid, plus the intravenous fluids that are given, increases patients' hydration to help dilute the radiographic contrast material they will receive and to help prevent any possible renal dysfunction.
The usual patient selection and preparation principles are used. Angiograms are most often longer and more involved than other types of radiologic interventions, and the patient may have to remain on the table for hours at a time. To obtain high-quality images, it is imperative that patients lie absolutely still; consequently, they are often kept in position with a variety of soft restraints, belts, and bands. Depending on the type of study, they may be asked not to breathe, swallow, blink, or wiggle their toes.
Angiography can be tedious and exhausting for patients. Their arms are most often secured at their sides with wristbands to prevent them from inadvertently touching the long catheters or contaminating the sterile fields. Patients usually require repeated small doses of intravenous sedation, and they often sleep for short periods. However, patient cooperation during contrast injections is essential, and they are awakened to be monitored and provided with instructions.
In the standard procedure, the catheter is positioned in a specific location in the chosen blood vessel, and then pressure injectors shoot radiopaque dye directly into the catheter. Multiple images can be obtained as the contrast agent is injected. Patients may perceive a very warm or even hot sensation in the local area or along the region being studied, but the feeling disappears rapidly. With each injection, the interventional radiologic technologist tells the patient what is going to happen, reminds him or her not to move, and reassures that the warmth will go away. If catheters are positioned in vessels near or in the lower abdomen or pelvis, patients may get the feeling that they are urinating as the contrast enters that area. They should know in advance that this feeling may happen as many patients become upset and frightened by the thought that they have been incontinent.
Abnormalities in blood vessels cannot be repaired or altered until their exact anatomy is ascertained. The procedure allows one to follow the flow of blood through the lumens and see which vessels branch off other vessels, which have strictures, and which have limited blood flow. By following the stream of dye through the veins and arteries, it is possible to see vascular occlusive disease, aneurysms, arteriovenous malformations, and arteriovenous fistulae, as well as to diagnose and localize small vascular tumors. Preoperative assessment of vascular anatomy is provided, which is essential before organ transplants, revascularization, bypass graft procedures, and certain tumor resections can be performed.
Angiograms aid in the diagnosis and treatment of vascular complications of disease or surgery and are a means by which interventional radiology teams can perform percutaneous vascular interventional procedures such as angioplasties, embolizations, and infusions of certain therapeutic medications. As noted, many therapeutic procedures are performed in the radiology department during angiography. A great majority of these procedures have replaced open surgery. Similar to biopsies and drainages, they can spare patients general anesthesia and days or weeks of hospitalization.
Before undertaking any angiogram, the interventional team should assess all the patient's pulses, including axillary, brachial, radial, femoral, popliteal, and dorsalis pedis. Pulses are checked by touch as well as by Doppler to establish a baseline for the postprocedure observation and also to assist the radiologist in selection of the point of entry for the angiographic needle. Arteries are often deep in the tissues, and optimal entry sites are located by assessing the patient's pulse points along with the knowledge of normal anatomy.
Because the circulatory system is closed, with vessels branching or extending one from another, it is possible to selectively catheterize a vessel. For example, the renal artery may be entered, studied, and repaired through an opening made in the femoral artery. The approach chosen depends on the area to be examined, the patient's condition, and the angiographer's personal preference. During the procedure, the team should be prepared to handle any emergency that may occur and should strictly adhere to all established protocols. Most hospitals use specialized informed consent forms for angiography, such as that shown in Table 6.
Angiography is a sterile operative procedure, with the room set up and the staff dressed in surgical attire (as in the operating suite). Preparation takes time because meticulous care is taken to be certain no air bubbles are present in injector systems, tubings, and catheters. Most angiograms are performed through arterial punctures, and air can be deadly in the arterial circulation. There are almost always some small air bubbles present in intravenous tubings, but this cannot be allowed during arteriography. Venous studies (e.g., a catheter placed in the femoral vein threaded up and through the heart to assess the subclavian vein) have their own potential dangers.
Femoral artery punctures are the usual arteriographic approach. Other approaches are the brachial or axillary artery and the translumbar approach, but these are used less often and only under specific circumstances. The common femoral artery is easily accessible, is fairly large, and has the lowest statistical complication rate (less than 0.5%) compared with translumbar (0.6%) and axillary (1.7%) approaches [77,78]. While the rates of major bleeding with femoral access have declined significantly over time, the transradial approach offers advantages of reduced vascular complications and length of stay and enhanced patient comfort and patient preference, while maintaining procedural success [79,80]. Moderate sedation is administered, and the radiologist finds the point of entry by palpating the femoral pulse. Local anesthetic is infiltrated subcutaneously, and the appropriate needle is used to catheterize the vessel.
When a hollow needle enters an artery, an immediate spurt of bright red blood results. Arterial bleeding is quite easy to differentiate from venous bleeding, both by the color of the blood and by the fact that it pumps rather than drips from the lumen of the needle. After cannulation of the vessel is accomplished, a guide wire is introduced. By means of fluoroscopic guidance, the catheter is inserted into the vessel over the guide wire. Unlike most other divisions of radiology, the interventional team should remain in the room with the patient during the entire procedure. Protective gear, such as lead aprons, thyroid shields, and eyeglasses, are worn at all times to protect the staff. A radiation dosimeter should be worn by all personnel involved in the angiographic procedure.
Arterial puncture site complications are rare and include thrombosis, arterial dissection, arteriovenous fistula, pseudoaneurysm, and hematoma, the last of which is most common [77,78]. Blood flow can be compromised during the procedure, resulting in ischemia, permanent organ damage, or death. As with any procedure, the benefit should be weighed against the potential risk of complications. While angiography in the hands of a qualified team is considered an extremely safe and advantageous procedure, no hospital should perform the procedure unless there is vascular surgery backup available should problems arise [81].
For decades, angiography has been an invaluable diagnostic tool for clinicians. The therapeutic applications of angiography have expanded greatly, with techniques including balloon angioplasty, femoral angioplasty, renal angioplasty, aortic angioplasty, and dialysis fistula and graft repair.
According to the American College of Cardiology, the American Heart Association, and the Society for Cardiovascular Angiography and Interventions, percutaneous revascularization is a reasonable option to improve survival, compared with medical therapy, in selected patients with low-to-medium anatomic complexity of coronary artery disease and left main disease that is equally suitable for surgical or percutaneous revascularization.
(https://www.jacc.org/doi/10.1016/j.jacc.2021.09.006 Last Accessed: June 1, 2022)Level of Evidence: Expert Opinion/Consensus Statement
Balloon angioplasty, also known as percutaneous coronary intervention (PCI), is a nonsurgical means to open blood vessels blocked by atherosclerosis or other causes. The procedure is performed following diagnosis of the blockage by angiography.
The principles of angioplasty in any vessel are basically the same. The procedure consists of guiding a balloon-tipped catheter into the narrowed vessel under fluoroscopic guidance and inflating the balloon, which breaks the atherosclerotic plaque, presses it back against the walls of the vessel, and opens the narrowed segment. PCI is most commonly performed in the arteries of the heart and legs, but also may be performed in the vessels of the arms, kidneys, or abdominal organs. Angioplasty may also be of benefit in opening areas of surgical grafts that have begun to stenose.
Stenosed arteries can cause many types of problems. In the legs, they can lead to symptoms of pain with exercise (intermittent claudication) or even gangrene. In the kidneys, they may produce high blood pressure and/or poor renal function. Abdominal pain may result from decreased blood supply to various organs.
PCI may be performed instead of surgical bypass grafting, but each case should be individually evaluated and diagnosed. Inflating and deflating the balloon several times along the area to be dilated enlarges the vessel lumen by disrupting the plaque and intima in a controlled manner. When arteriosclerotic disease involves extensive segments of blood vessels, balloon angioplasty may not be feasible as it may be impossible to open large areas of a vessel with the standard equipment.
Certain drugs may be used before and at the time of balloon angioplasty. When there is a tight stenosis or stricture, it often becomes difficult to pass the wire through the narrowed portion of the vessel. The physician performing the procedure may ask the nurse to administer sublingual nifedipine, which results in vasodilatation and reversal of vasospasm when absorbed under the tongue. This may open the blood vessel just enough to allow passage of the wire and catheter. A small dose of intra-arterial nitroglycerine, administered directly into the artery by the physician at the point of the stenosis, will usually work along with the nifedipine to open the vessel. Tolazoline hydrochloride may be administered into the artery at the point of the vasospasm and usually opens the vessel enough to allow the stricture to be bypassed. As with any vasodilator, the staff should watch carefully for a drop in blood pressure and be ready to institute any measures necessary to maintain a steady pressure. Intra-arterial or intravenous heparin may be given as a bolus dose as the stenosis is crossed, both for its anticoagulant and antispasmodic effects.
While PCI is a safe and effective treatment for short vascular stenoses and occlusions, it is not without a small risk of potential problems, including reaction to the intravascular contrast media, a chance of renal failure, or vascular injury related to the catheterization itself and direct trauma caused by the balloon. Balloon angioplasty also gives a greater chance of acute arterial dissection, thrombosis, or distal embolization by the directed focal trauma it induces, as well as by the larger hole required at the percutaneous entry site. Rarely, the dilated artery may even rupture. There is also the potential for some of the arteriosclerotic plaque or small blood clots to break away and cause obstruction of blood flow farther along the path of flow through the vessel.
It should also be noted that vessels opened by PCI may begin to restenose. Repeat procedures may be indicated after a certain period of time, but the advantages of the procedure are potentially great [82,83,84].
Balloon angioplasty of the lower extremity is a common site for interventional radiologic PCI. The procedure is indicated for stenoses resulting in intermittent claudication, general extremity pain, nonhealing ulcers or gangrene, preoperative reasons, or restenosis of a previous graft anastomosis.
The approach is most often through the common femoral artery and is best accomplished by entering on the opposite leg. The catheter is threaded up and around the aortic bifurcation and down into the iliac or femoral artery of the involved leg to the point of the stenosis that has been documented on angiogram. Balloon catheters come in different sizes, and their choice depends on the size of the vessel as well as that of the stenosis. Balloons have radiopaque markers that are used to assess their position in the blood vessel under fluoroscopy. The balloon portion of the catheter is advanced over a guide wire into the affected area of the vessel so that the radiopaque markers appear at both ends of the stenosis.
When the balloon is in the correct position inside the occlusion, it is inflated with a mixture of sterile saline and contrast medium. Besides allowing the procedure to be watched under fluoroscopy, this is also a safety measure because both the contrast and saline would be observed in the circulation if the balloon should break.
During balloon inflation, it is possible to visualize an hourglass shape in the narrow area and see the "waist" give way and the balloon become "sausage-like" in appearance. This is documentation of the stenosis being dilated. The balloon is kept inflated for an average of 20 to 40 seconds. It is not unusual to have to perform several inflations before the stenosis "gives" and the vessel is adequately dilated. When the vessel appears dilated to the appropriate size, another angiogram is performed to document and verify the results.
Lower extremity PCI provides good results and usually relieves the claudication that has limited the patient's activities. This type of therapy may be much preferred by patients as well as physicians instead of bypass surgery and may relieve obstructions in the femoral, iliac, or popliteal arteries, bringing symptom relief as far down as the knee.
Patients with strictures in the renal arteries experience hypertension, and many can be helped by renal artery angioplasty. Some of these patients have had high blood pressure and have taken antihypertensives for years. Finding and opening areas of stenosis in the renal arteries often reduces or even eliminates the need to continue medication. The procedure may also be indicated for patients with severe renal vascular disease and renal insufficiency and may result in a marked increase in the quality of life for these individuals.
Pressure gradients may first be measured across the renal artery stenosis and percutaneous transluminal angioplasty accomplished in the same manner. Because vascular spasm with renal artery PCI may be a more difficult problem, these patients are more likely to be given vasodilators. Because they usually already have blood pressure problems, they should be watched closely. In addition, many of these patients have borderline kidney function and require extra hydration and diuresis to prevent any type of insult from the intravascular contrast material. Overall, patients who undergo renal artery angioplasty have lasting morphologic improvement in the lumen of the dilated vessels.
Although most patients undergoing balloon angioplasty of other vessels are discharged the same day, this is not usually the case with renal artery angioplasty. There can be great fluctuations in blood pressure after the stenosed artery is opened, and patients are frequently monitored on nursing units for the first 24 to 48 hours. Formerly high blood pressure ordinarily stabilizes, and patients are usually ready to leave the hospital after this time.
The abdominal aorta often suffers from occlusive disease, much as other vessels of the body. Most often the stenosis is at the bifurcation of the aorta, which may be quite amenable to transluminal angioplasty. Naturally, because the walls of the aorta are constantly under great stress from the great volume of blood that it handles, there is always a chance of rupture from the added pressure of the balloon. However, with good patient selection and an experienced operator, patients do well, and some studies show that bifurcation stenoses can be opened in more than 90% of cases and remain open for at least a year [85].
The number of patients undergoing hemodialysis for chronic renal failure has increased dramatically in recent years, mainly due to the surge of type 2 diabetes cases. Maintenance of vascular access in these patients may present major problems. Permanent peripheral hemodialysis access can be created by direct anastomosis of a vein to the side of an artery to create a fistula or by placement of a graft bridging the artery and vein. Over the years, many changes have evolved in the materials with which grafts are constructed, from animal veins and human umbilical veins to synthetic materials. Today, grafts are most often synthetic types. There are many potential problems with dialysis fistulas and grafts, the most common of which is stenosis caused by venous anastomotic intimal hyperplasia (VAIH).
Most stenoses in dialysis access shunts resulting from VAIH are caused by the turbulence and stress of high-volume blood flow. Problems manifest themselves as poor flow, changes in pressure, and notable increased resistance during the dialysis procedure. Occlusions may come from stenoses, various low flow states, or other etiologies. Many authorities feel that angiography should be performed at the first sign of graft or fistula dysfunction.
Percutaneous angioplasty to restore patency may be performed through the graft itself, through the veins in the arm, or through a femoral venous approach. Strictures at venous anastomoses may be particularly severe and successful dilation often requires prolonged inflation with high-pressure balloons. During these procedures, patients may require extra doses of intravenous analgesics and sedatives.
Because clots often form in occluded grafts, repair often involves a combination of procedures. After PCI is used to break through the scar tissue forming the stenosis, mechanical thrombectomy devices may be passed to literally pulverize and aspirate blood clots. Some clinicians also use thrombolytic agents such as recombinant tissue plasminogen activator (rt-PA) to lyse, or dissolve, the clot over a short period of time. During these procedures, heparin and aspirin therapy may be administered concurrently.
Some studies have found that although early response tended to be good, some patients had a tendency to develop intimal hyperplasia and recurrent stenoses. However, fistula or graft PCI can be repeated with good results, sparing patients invasive surgical procedures to replace dialysis shunts [86]. One study has shown that primary patency with PCI was 82.4% over three months; 81.2% over six months; 54.5% over nine months; and 50% over one year [87]. Intravascular stents may be placed in areas of restenosis.
Vascular stents are commonly used to improve the result of balloon angioplasty. They act as a scaffold to hold the vessel open, preventing elastic recoil. Stents are usually made of metallic coils or tubular mesh and are introduced into the vessel by a delivery catheter. The goal is to have the endothelium of the blood vessel grow and cover the surface of the stent, which helps to protect it against low-flow thrombosis.
The stent is directed to the desired location by an introducer catheter and then deployed into position. Wallstents are commonly used. They are self-expanding and flexible, allowing deployment in curved vessels or from contralateral approaches. As long as the Wallstent has not exceeded the deployment threshold, it may be withdrawn or removed if positioned unsatisfactorily. The Palmaz stent, a balloon mounted radiopaque stent, is also used for peripheral vascular implantation.
Vascular stents come in various sizes and lengths and have increased the success rate of various types of percutaneous transluminal angioplasty. In some larger medical centers, interventional neuroradiologists are performing carotid stenting, avoiding standard carotid endarterectomy.
It has been estimated that in simple lesions the incidence of restenosis of a bare-metal stent is in the range of 17% to 41 [88]. It can be considerably higher for more complex lesions.
Several modalities have been suggested to help reduce the incidence of restenosis or to treat an occluded stent. These include stents that elute medications, such as sirolimus, balloon angioplasty, and transient brachytherapy with a source of radioactive material. It appears that sirolimus-eluting stents result in a better outcome [89,90,91,92,93]. Despite the continued improvement of drug-eluting stent technology, treatment of stent restenosis remains challenging due to its multifactorial etiology [94].
There are many stents available that are tailored to specific areas of the vascular system and made from a variety of materials. Vascular stents are contraindicated in patients with bleeding disorders, in instances when placement of a stent could exacerbate arterial leakage, when a patient cannot take blood thinning medications, and when stenoses cannot be dilated to allow passage of the delivery catheter; additionally, some patients may have an allergy to certain stent materials (e.g., nickel-titanium alloy) [95,96].
Filters may be placed in the inferior vena cava (IVC) of patients who are prone to recurrent episodes of pulmonary emboli (PE). Most of these patients have been treated with standard anticoagulants and have either not responded or cannot continue the therapy. Retrievable filters are sometimes placed prophylactically in certain high-risk patients with trauma, such as severe closed head injury with a Glasgow coma score less than 8, spinal cord injury with paraplegia or quadriplegia, or complex pelvic fracture with associated long bone fractures; individuals with these traumas who cannot receive anticoagulants or who are older than 55 years of age are considered high-risk for PE or deep venous thrombosis (DVT) [97]. Incidence of DVT and PE may be as high as 25% and 32% respectively for these patients [98].
Wire frame or metal mesh filters are placed in the IVC to prevent clots that have formed in the lower extremities from ascending to the lungs. The filter traps the clots, and then the patient's natural lytic system dissolves them. The Greenfield filter is a commonly used IVC filter and has the appearance of a tiny umbrella when deployed [99]. If there is a clot in the IVC itself, the Greenfield filter may be placed above the renal vein with much less risk to renal function. Another commonly used filter is the "bird's nest filter," named for its tangle of wires. All IVC filters are inserted through the skin into a vessel and advanced up to the desired site. After proper position is determined, the filter is opened and the wire is removed. No attempt is made to move the filter after it is deployed due to the chance of vessel perforation [99]. Several retrievable filters have been FDA-approved for use in the past decade, including the Günther Tulip filter, the G2/G2 and G2 X filters, the OptEase filter, and the Celect filter (based on the Günther Tulip filter). These devices are sometimes referred to as optional filters because they can be retrieved after a period following placement or can be left in the patients as a permanent device [99].
If the IVC filter is permanently placed, careful consideration and patient assessment should precede the intervention to determine if it is the best option. The use of a permanent filter requires lifelong anticoagulation; this has raised the question of whether it is prudent to place permanent devices in patients younger than 55 years of age.
Retrievable filters have become more common, especially when used as prophylactic treatment. The Society of Interventional Radiology guideline recommends that the decision to use retrievable filters be based on the "anticipated required duration of protection against clinically significant PE and/or risk of pharmacologic therapy" [100]. While IVC filters remain the only treatment option for patients with an acute (within two to four weeks) proximal DVT or PE and an absolute contraindication to anticoagulation, there is insufficient evidence to support the use of IVC filters for other indications [101,102]. Anticoagulation should be resumed and IVC filters removed as soon as the contraindication has passed [102,103,104]. In 2014, the FDA issued a safety communication regarding retrievable IVC filters, based on reports of adverse events and product problems [103]. The types of adverse events reported included device migration, filter fracture, embolization, perforation, and difficulty with filter removal. The FDA found that these types of events may be related to how long the IVC filter has been in place and recommends that implanting physicians and clinicians consider removing the filter as soon as protection from pulmonary embolism is no longer needed [103]. Despite the substantial rates of complications associated with retrievable IVC filters, a high proportion of them are not removed [104]. The femoral and jugular veins are the two standard approaches used in placing IVC filters. The femoral approach is used more often because there is no need to maneuver an angiographic catheter through the heart. The filter is guided up through the femoral vein to the iliac vein and positioned in the IVC. It is important to be certain that there are no clots in the femoral or iliac at the time of the insertion because the installation of the filter could theoretically dislodge the clot and push it up toward the heart. The possibility of blood clots being present in the legs is usually checked by means of ultrasound. If any are shown to be present, the jugular vein approach may be used.
It is important to check the angiogram carefully to make certain that the positioning of the filter is below the renal veins. At the same time, it is possible to ascertain if the size of the filter is appropriate for the patient's anatomy. If the jugular approach is taken, the radiology staff should be alert to changes on the cardiac monitor as arrhythmias may occur as the filter is guided through the heart.
Hemorrhage and thrombus are the largest risks from IVC filter placement and can develop in a traumatized vein. In addition, a smaller risk exists for perforation of the vessel. Some surgeons insert vascular filters in the operating room under general anesthesia, but interventional radiology spares the patient a greater ordeal and usually provides the same result. IVC filter placement can be of great benefit to the patient. It is effective in reducing or preventing potentially life-threatening pulmonary emboli.
According to the American Society for Gastrointestinal Endoscopy, most studies have shown only minimal relief of the intensity and duration of pain from celiac block in patients with chronic pancreatitis. Systematic reviews estimate that celiac block provides pain relief in 51% to 59% of those, but the relief is temporary, typically less than 24 weeks in duration. Limited data suggest that endoscopic ultrasound-directed celiac block is more effective, less expensive, and preferred by patients compared with CT-guided therapy, but the methodologic limitations limit firm conclusions.
(https://www.giejournal.org/article/S0016-5107(15)02381-0/fulltext Last Accessed: June 1, 2022)Level of Evidence: Expert Opinion/Consensus Statement
CT-guided celiac plexus block is considered to be a fairly permanent and safe method of pain control. It is primarily used for the relief of intractable pain in patients with malignant abdominal disease or for the relief of chronic, severe visceral abdominal pain in certain types of benign disease, such as chronic pancreatitis.
The celiac plexus is a dense network of sympathetic nerve fibers coursing along the anterior surface of the upper abdominal aorta. It serves as a relay station for visceral afferent nerve fibers that carry pain sensation. The plexus block is performed with sterile ethyl alcohol (or alternatively, phenol), which anesthetizes the nerves that conduct pain. As a result, the patient can become pain free and will no longer need continuous analgesics to maintain some degree of comfort; however, permanent relief may require several treatments.
Patients are usually given IV moderate sedation for both comfort during the procedure and to minimize the psychologic aspect of long needle insertion. The procedure itself involves the insertion of long, hollow, 18- to 22-gauge needles directly into the specific areas affected. A test injection of a small amount of air or contrast medium (5 mL) assures that the needles are correctly positioned. Typically, 20–50 mL of ethyl alcohol is then injected through the same needles. An anesthetic (e.g., lidocaine, bupivacaine, levobupivacaine) may be instilled at the same time because it can be painful when the ethanol is injected into the area. Afterwards, puncture sites are covered with simple bandages. Patients are kept on bed rest for approximately eight hours and are watched for transient hypotension, which can result from loss of visceral vascular tone. If all goes well, patients can be discharged the next day with a greatly improved quality of life.
While the field of pain control is growing rapidly and many anesthesiologists manage much of the severe pain that debilitates so many people, most celiac blocks are performed in radiology departments, using CT guidance. Radiologically guided plexus block also has the advantage, over "blind" blocking, of greatly reduced instances of complications such as paralysis and sexual dysfunction.
Embolization is a procedure that has become more common in clinical practice. It is used to form a thrombus in order to block the flow of blood in a vessel. Using the human body's natural tendency to form a clot over a foreign body in a vessel, this technique can be used to close an arteriovenous malformation (AVM) or stop a hemorrhage. It can also decrease vascularity and lessen pain caused by the bulk and position of tumors and may be indicated for some aneurysms.
Making a choice from the numerous materials or agents available for use in embolization procedures depends on the objective of the therapy. Angiography is performed and selected types of particles are instilled into the vessel and deposited exactly at the location that is to be treated with fluoroscopic guidance. Fibered coils, tiny pieces of Gelfoam, balloons, and metallic "spiders" are types of materials that may be used in embolic therapy. After these materials reach their target areas, the body begins to seal the area around them naturally, blocking blood supply to the involved site.
Follow-up angiography shows the difference in the area being treated. Before and after images may show a dramatic decrease in blood flow. Examples of conditions that benefit from embolization therapy include uterine fibroids, gross hematuria from kidney tumors, massive hemoptysis from pulmonary AVM, epistasis, and trauma [105,106].
The staff that cares for these patients should be aware of postembolization syndrome, including pain, nausea, vomiting, and fever, which virtually all patients experience, in varying degrees. These symptoms tend to be self-limiting, and therapy is supportive. Embolization for the treatment of uterine fibroids has become one of the more common uses of the technique and will be discussed as an example of the procedure.
Until recently, the standard treatment options for uterine fibroids have been myomectomy or hysterectomy, the definitive cure. However, surgery is not an option for many women, so they continue to bleed heavily during their monthly cycle.
Interventional radiologists have pioneered the use of uterine artery embolization as a treatment for symptomatic uterine fibroids. By occluding flow in the right and left uterine arteries, the fibroids are deprived of their blood supply. This leads to necrosis, degeneration, and eventual infarction of the fibroid, which results in a dramatic decrease in abnormal uterine bleeding and bulk-related symptoms [107].
Under moderate sedation and local anesthesia, the right or left femoral artery is punctured and catheters are guided into both uterine arteries. The uterine arteries are embolized with tiny polyvinyl alcohol particles, a fixative, and then a final angiogram is performed to confirm that there is no longer blood flow in the uterine arteries. Patients who undergo this procedure may experience cramping and are prophylactically medicated for this.
There have been studies and reviews to determine whether bilateral embolization is always necessary if fibroids are limited to one side of the uterus and are supplied by only one uterine artery. Some consider unilateral embolization to be effective, producing less postoperative pain and providing a greater margin of safety [108]. Other researchers point to the greater incidence of further interventions required, including hysterectomy, after unilateral embolization as proof that bilateral embolization should be standard practice in all cases [109].
A Cochrane review (that did not address unilateral versus bilateral embolization) did find that overall patient satisfaction was similar between embolization and hysterectomy or myomectomy and that embolization resulted in a shorter hospital stay and a faster return to routine activities. However, embolization was associated with a higher rate of minor complications and an increased likelihood of requiring surgical intervention within two to five years of the initial procedure [110].
Women should understand that it will take several months until the fibroid size decreases and results are realized. In addition, infertility may be a problem for some women undergoing this procedure because embolization significantly reduces the amount of blood available to the uterus during pregnancy. Restoration of uterine anatomy and ovarian protection have been identified as main predictive factors of obstetrical success [111]. Patient education is vital before any patient undergoes uterine artery embolization.
Along with an increasing knowledge of the mechanisms of atherosclerosis and vascular stenosis has come an increasing number of procedures and techniques for diagnosing and treating the conditions. An example is carotid artery ultrasound, used in the early detection of atherosclerotic lesions [112].
As previously mentioned, interventional radiology provides methods of treating stenosed regions, primarily with angioplasty and stents. In addition, where emboli may be the cause of the vascular blockage, emboli retrieval devices can be inserted transvenously to remove the course of the ischemia [113].
Many more individuals are now receiving dialysis. Patients with dialysis grafts and temporary dialysis catheters may develop stenoses in the central veins, such as the large veins in the thorax and neck. Subclavian vein stenosis is not uncommon and may be successfully angioplastied and/or stented. To reach the subclavian vein, it is necessary to enter through the femoral vein and thread the guide wire up the iliac vein to the inferior vena cava and into the right atrium of the heart. The wire is moved through the atrium and out into the subclavian vein.
When the wire passes near the heart, it may loop into the right atrium and "jiggle" against the junction to the ventricle. During this time, the staff should be alert to changes on the cardiac monitor because it is at this point that runs of potentially lethal ventricular tachycardia may develop. It is important to pay close attention to the cardiac rhythm so that the offending guide wire can be adjusted.
Peripherally inserted central catheters (PICC lines) are frequently used in patients requiring long-term intravenous therapy. These lines spare the patient from longer and more invasive procedures to place implanted ports.
PICC lines are long, thin venous access devices with single or double lumens that are inserted into the basilic or cephalic vein and threaded into the central circulation, most commonly the superior vena cava or right atrium. Antibiotics, narcotics, and total parenteral nutrition (TPN) are some of the long-term therapies given via PICC lines.
Although certified IV therapy nurses insert many PICC lines, interventional radiologists may perform the procedure under fluoroscopic guidance to ensure adequate catheter placement, especially in difficult or critical situations. In the past, verification may have necessitated several adjustments, x-rays, and calls to radiology.
Endovascular grafting is an accepted, minimally invasive procedure being used in many medical centers for selected patients who require repair of an abdominal aortic aneurysm (AAA).
Growth of an AAA larger than 6 centimeters is associated with a 30% chance of rupture within one year. Traditionally, an abdominal aortic aneurysm is repaired by a major abdominal surgical procedure, which replaces the aneurysmal part of the vessel with an anastomosed prosthetic graft. This procedure usually necessitates a hospital stay averaging 5 to 10 days.
A pioneering endovascular technique was introduced in 1991 in which a sutureless vascular graft is inserted and implanted into the abdominal aorta through a femoral arteriotomy. An abdominal incision is not needed and the postoperative course typically requires only one to three days of hospitalization in a general medical-surgical nursing unit.
With this procedure, a vascular surgeon is usually present, working with the interventional radiology team. General anesthesia is most often used. Endovascular graft placement may be performed either in the operating room or in an interventional radiology room [114].
Early results of endograft implantation were disappointing owing to graft design; however, built on experience, the new prostheses (e.g., Talent, Zenith, Endurant) are more durable and less prone to leakage, kinking, and migration, making this procedure a safe and effective alternative to open surgery for many patients [115,116,117]. The early survival benefit of endovascular abdominal aortic aneurysm repair is sustained up to three years postoperatively, but longer-term life expectancy remains poor regardless of operative modality [118]. However, it is not an option for some, including patients with smaller femoral arteries. Additionally, there is an increased risk for artery damage with the use of the procedure.
Percutaneous pulmonary valve implantation (PPVI) and percutaneous aortic valve replacement (PAVR) are another set of newer but proven effective alternatives to open surgery. Often, patients are at too high an operative risk or have substantial comorbidities, making a full sternotomy not an option. There are substantial complications that can arise from cutting and spreading the sternum and bypassing and stopping the heart, including elevated creatinine levels, bleeding, stroke, and impaired lung function. Additionally, patients are spared lengthy recoveries and extensive or abnormal scarring with percutaneous cardiac interventions.
An artificial valve, most often constructed from an equine or bovine jugular valve sewn onto a metal stent, is housed in the delivery catheter. Aortic replacements are threaded through the femoral vein with a transseptal approach across the mitral valve to the left ventricle or antegradely through the femoral/iliac or subclavian artery to the ascending aorta [119]. Pulmonary replacements are advanced through the femoral vein and are placed within the existing pulmonary valve. The heart remains beating throughout the procedure, which is performed using fluoroscopic guidance with the patient generally anesthetized.
Since the first PPVI procedure in 2000 and the first PAVR in 2002, results have been favorable for the continued use of these interventions on specific high-risk patients and perhaps warrant use in other groups as well [120,121,122,123,124]. As experienced with AAA grafts, first-generation replacement valves may have had design issues and have subsequently been re-engineered. Trials have shown that if early device failure occurs, repeat percutaneous implantation is safe and effective and, in most instances, will provide the patient with improved freedom from re-intervention within two years; percutaneous replacement, in general, will likely reduce the number of interventions needed over the total lifetime compared with conventional replacement [121,124]. A study that compared psychosocial function and clinical outcomes following surgical intervention and PPVI at three months and one year after treatment found that both methods led to clinical improvement. Thought and attention problems (e.g., intrusive behavior) significantly decreased only in patients who underwent the PPVI procedure; complications such as reintervention, bleeding, and arrhythmia were observed only in the open surgery group [125]. One meta-analysis has found that mortality is not linked to PAVR device failure but to associated cardiovascular disease instead [126]. These findings are likely corollary to PPVI as well.
Transjugular intrahepatic portosystemic shunt (TIPS) is a nonoperative therapeutic option for management of variceal bleeding that results from portal hypertension. The portal system is that part of the systemic circulation that is distinguished by the fact that blood from the spleen, stomach, pancreas, and intestines first passes through it before exiting the liver.
Two major blood vessels supply the liver, with about one-third of the blood supply coming from the hepatic artery. Two-thirds comes from the mesenteric and splenic veins through the portal vein, bringing nutrients and metabolic substances from the stomach and intestines. After processing the blood, the liver releases it to the systemic circulation through the hepatic veins and into the inferior vena cava.
When a patient develops cirrhosis, the flow of blood backs up through the liver and follows the path of least resistance into the veins that normally drain the stomach and intestines. The esophageal and gastric vessels reroute the blood from the high-pressure system in the liver and carry it through a low-pressure system into the systemic circulation. With cirrhosis, these vessels begin to enlarge and become tortuous. These varices often begin to leak, and the patient develops ascites in addition to possible bleeding disorders and hepatic encephalopathy.
Results can be catastrophic when esophageal varices bleed because the vessels are large and under pressure. A patient can lose large volumes of blood and quickly go into shock. Treatment involves restoring blood volume, administering drugs that temporarily decrease portal system blood flow, administering sclerotherapy to the bleeding points of the varices, and tamponading the bleeding varices. This is performed with large nasal tubes such as Sengstaken-Blakemore or Minnesota tubes, which are often configured to provide direct pressure with the gastric and esophageal balloons. These are only temporary measures.
Portal decompression can be obtained by shunting the blood, which is performed by a surgically created portosystemic shunt. This is major surgery with a relatively high mortality and morbidity rate for the critically ill patient. TIPS is an interventional radiologic procedure that is an alternative to the other medical and surgical therapies. With this technique, the normal vascular anatomy of the liver is used to create a shunt between the portal and systemic venous systems entirely within the liver, using a metallic stent or expanded polytetrafluoroethylene (ePTFE) stent-graft to relieve portal hypertension.
Before preparations for this procedure are finalized, patients usually undergo ultrasound Doppler studies of their portal and hepatic vessels so that their particular anatomies will hold no surprises for the interventional radiology team. TIPS is relatively noninvasive, requiring only a puncture in the jugular vein, which is followed by a guide wire and catheter manipulated into the hepatic vein of the liver under fluoroscopic or other guidance. A transjugular needle follows the same pathway. A dilated tract is created through the liver itself, forming a shunt from the portal vein to the hepatic vein. At this point, a stent is placed in the newly formed tract and expanded, creating a portosystemic shunt entirely within the liver. One study found that shunts created with ePTFE stent-grafts had better primary patency and clinical success rates than those created with metal stents [127].
Another study found construction of a TIPS with either a single stent-graft or bare metal stent-graft combination effectively controlled variceal bleeding and that the combination technique was superior to the stent-graft technique in terms of preservation of hepatic function. The two techniques were comparable in terms of primary shunt patency, incidence of encephalopathy, and patient survival during long-term follow-up [128]. An evidence-based review suggests that selection of the appropriate stent for TIPS procedures should be the focus of future studies, with emphasis given to stent size, which may improve survival and shunt patency; whether the stent is covered or bare, which affects shunt patency; and stent placement, which may help decrease the development of hepatic encephalopathy [129].
The TIPS procedure can be quite painful, so patients require moderately high doses of moderate sedation. Patients are positioned on fluoroscopy tables in a slight Trendelenburg position and may have to remain that way for several hours. Many facilities routinely provide general anesthesia to keep patients comfortable.
Hemorrhage and bile duct trauma are the major complications from TIPS. Serious problems can result from laceration of hepatic arteries or the liver tissue itself during attempts to puncture the portal vein. A patient undergoing a TIPS procedure is subject to many other problems. However, when the procedure is over, portal pressure drops and variceal bleeding should stop.
Patients who undergo TIPS procedures generally do very well. Like surgery, TIPS corrects the problems as opposed to simply managing the symptoms. But unlike surgery, it carries a much lower mortality and morbidity rate. TIPS patients are usually discharged within two to four days postprocedure [130].
Radiofrequency ablation (RFA) is a percutaneous procedure that uses radiant energy to treat tumors. The objective of this therapy is to produce enough heat to literally cook and kill the tumor. The body eventually absorbs the damaged tissue, leaving a scar in its place. RFA may be performed in conjunction with radiotherapy and/or chemotherapy. Originally used to treat tumors of the liver, the procedure is expanding in scope and has been used for treating lesions in other organs. Small renal and adrenal tumors, lung cancers, and even osteoid osteomas have been successfully ablated with RFA [131].
Imaging guidance to accurately locate the lesions is usually accomplished with CT or ultrasound. A follow-up study with CT, MRI, PET, or ultrasound is generally required to determine the success of the procedure. When CT is used for imaging, gas produced by RFA obscures the site and follow-up studies are necessary. Technologies for determining the outcome of the procedure while it is being performed are in development [132,133,134,135].
Patients are usually given IV moderate sedation for the procedure. A grounding pad is applied to the patient, and local anesthetic is injected. With appropriate imaging guidance, a specifically designed needle-electrode, attached to a RF generator, is inserted into the center of the lesion. The treatment begins when the target temperature is reached (60 to 100 degrees C). The tumor is heated for 7 to 15 minutes, on average, which is enough time to kill the cancerous cells and a 1-cm margin around the tumor. The entire procedure can take up to four hours. As the needle is retracted and removed, the probe maintains a burn temperature so that the tract will not be seeded with tumor. Smaller lesions (less than 3 cm) appear to have a better success rate than larger tumors [136,137]. New image-guidance tools and devices being prototyped and investigated will enable radiologists to more accurately target the more challenging biopsy and ablation targets [132]. Postprocedure nausea, vomiting, fever, and pain are common after this procedure and are considered the body's reaction to the damaged tissue. Serious complications include pneumothorax and hemoptysis.
Microwave ablation is an extension of RFA technology, using a higher energy segment of the electromagnetic spectrum that essentially applies the same principles as microwave cooking to treating tumors. Several limitations of RFA exist that relate to heating capability and, therefore, tumor killing ability, which are overcome by microwave ablation. First, RFA heat generation relies on conductivity between the needle-electrode and grounding pad; as the temperature of the electrode approaches 100 degrees C, soft tissue begins to vaporize and conductivity is diminished; thus, heating stops until the tissue rehydrates and the electrode can be turned back on. Second, blood circulation around the treatment area cools the tissue oftentimes faster than the RF electrode can generate heat [138]. Rather than using electrodes (i.e., needle and grounding pad), the microwave needle-antenna is self-radiant and does not rely on conductivity; additionally, microwaves are higher energy than RF and capable of the intense molecular excitation needed to overcome the circulatory cooling effect. Microwave ablation offers the promise of treating larger tumors, with higher temperatures, faster ablation time, and an improved convection profile over RFA [138,139]. A five-year review of 270 microwave ablations found the treatment to be safe and effective, with a low rate of local recurrence (2% at 36 months); tumors up to 6 cm were successfully treated [140]. A comparison of high-frequency (2450 MHz) and low-frequency (915 MHz) microwave ablation devices found that high-frequency ablations resulted in larger ablation margins and fewer local tumor progression, based on follow-up CT, than low-frequency ablations [141].
In recent years there have been many breakthroughs in interventional radiologic intravascular drug therapy. Medications can be infused through indwelling catheters positioned deep in major arteries at the exact location of the problem, so the drug is instilled directly into the lesion or area involved.
Because they are infused at precisely the desired location, arterially administered medications cause an effect quite different from those given intravenously and systemic reactions can usually be prevented. The use of interventional intravascular drugs also helps to shorten hospital stays, providing patients with meaningful therapy through minimally invasive means.
While there are dozens of medications used for multiple purposes, three procedures have been selected as examples of what can be accomplished: thrombolytic therapy, vasodilation, and vasoconstriction (Table 7).
INTERVENTIONAL INTRAVASCULAR DRUG THERAPIES
| Drug | Therapeutic Category | Action | Indication | Contraindications | Adverse Effects |
|---|---|---|---|---|---|
| Alteplase (rt-PA) | Thrombolytic | Dissolves blood clots | To dissolve intravascular thrombi | Any recent surgery, trauma, intracerebral arteriovenous malformation (AVM), tumor, severe hypertension, left heart thrombus, diabetic hemorrhagic retinopathy, bleeding disorder | Bleeding (local or systemic) |
| Papaverine hydrochloride | Vasodilator | Causes relaxation of smooth muscle | To relieve vascular spasm, ureteral, biliary, or gastrointestinal colic and ischemia | Complete heart block, acute angle glaucoma | Hypotension caused by systemic vasodilation |
| Vasopressin | Vasoconstrictor | Causes contraction of smooth muscle | To control gastrointestinal bleeding | Coronary artery disease | Chest pain, angina, myocardial thrombosis, water intoxication (all caused by systemic vasoconstriction) |
The potential of recombinant tissue plasminogen activator (rt-PA), or "clot buster" drugs, is well documented. The public is taught the importance of getting people who experience chest pain or stroke symptoms to a hospital emergency room as soon as possible. An arsenal of drugs is available in emergency rooms and chest pain centers that, when given in time, can save tissues from permanent damage by dissolving clots and restoring circulation. This type of therapy can be used to lyse blood clots that obstruct blood vessels elsewhere in the body, such as the lungs and limbs.
One rt-PA used for the management of arterial occlusions is alteplase, an enzyme that enhances the conversion of plasminogen to plasmin, which initiates local fibrinolysis with limited systemic proteolysis. Other thrombolytic agents that have been used include streptokinase (the first medication for myocardial infarction, introduced in 1958), urokinase (more widely used in the past), reteplase, tenecteplase, and anistreplase. The American College of Chest Physicians published a study in 2004 in which they compared most of these agents for their use in treating patients with acute myocardial infarction. For patients with symptom duration of more than six hours, alteplase is recommended over streptokinase [142]. In the same year, an evidence-based report stated that an IV rt-PA given within six hours of suggested stroke symptoms could provide beneficial results, including fewer long-term deaths and less dependence in the activities of daily living, despite the increase in initial fatalities [143]. The conclusions stated in this report were reaffirmed in 2009 [144]. The 6-hour timeframe has since been revised, and rt-PA has been found to be highly effective if administered within 3 to 4.5 hours [145,146,147,148]. However, there are limitations regarding patient selection. Administration of rt-PA is contraindicated in individuals with a systolic blood pressure greater than 185 mm Hg or a diastolic blood pressure greater than 110 mm Hg [145,146,148].
It should be noted that the risk/benefit ratio becomes unfavorable when alteplase is administered more than three hours after acute ischemic stroke; therefore, if the onset of stroke symptoms is greater than three hours or is unknown, treatment with this agent is generally not recommended [20,145,149]. The primary risk of alteplase treatment is intracerebral hemorrhage, and there are many contraindications for alteplase, including history of intracerebral hemorrhage, recent previous stroke (within three months), recent head injury, recent surgery, uncontrolled hypertension, seizures, active internal bleeding, or rapidly improving or minor stroke symptoms [146,148,149]. Despite the conventional 3-hour efficacy and safety window, the third European Cooperative Acute Stroke Study (ECASS III) has shown that, although it is optimal to begin treatment as early as possible, there are still modest benefits gained 3 to 4.5 hours after onset of a stroke if presentation is delayed [146,148,150]. While there was an increased incidence of intracerebral hemorrhage in the 3 to 4.5 hour ECASS III treatment (versus placebo) groups, the hemorrhage rate was no greater than current 3-hour treatment statistics; mortality was also not greater [150]. Other research supports extending the approved treatment window to 4.5 hours, but likewise, stresses the importance of beginning treatment as early as possible [146,148,151,152,153].
The novel drug desmoteplase, a recombinant form of the plasminogen activator DSPAα1, derived from the saliva of the common vampire bat, Desmodus rotundus, is being investigated in clinical trials for IV treatment of acute ischemic stroke in the 3- to 9-hour window. While results of initial safety trials (Desmoteplase in Acute Ischemic Stroke [DIAS]; Dose Escalation of Desmoteplase for Acute Ischemic Stroke [DEDAS]) showed positive results up to nine hours after the onset of symptoms, the DIAS-2 phase III trial was unable to show any benefit after three hours, although this was possibly attributable to poor trial design [152]. The DIAS-3 and DIAS-4 trials are underway to prove benefit up to the 9-hour mark despite the indication that tissue damage is likely permanent after 4.5 to 5 hours [152]. Recruitment into the DIAS-4 trial was ended prematurely due to disappointing results from DIAS-3; the manufacturer subsequently discontinued its development for use in ischemic stroke [154; 155; 156].
Intra-arterial rt-PA can be used as a thrombolytic agent following angiographic demonstration of intravascular thrombi. Because of the extreme potency of this agent, there are many contraindications for its use. Even though it is infused through a catheter that is angiographically placed at the site of the thrombus, it may be systemically absorbed. Because there is a real potential for bleeding, patients who receive this drug should be thoroughly screened. Most often this is completed by means of a checklist (Table 8).
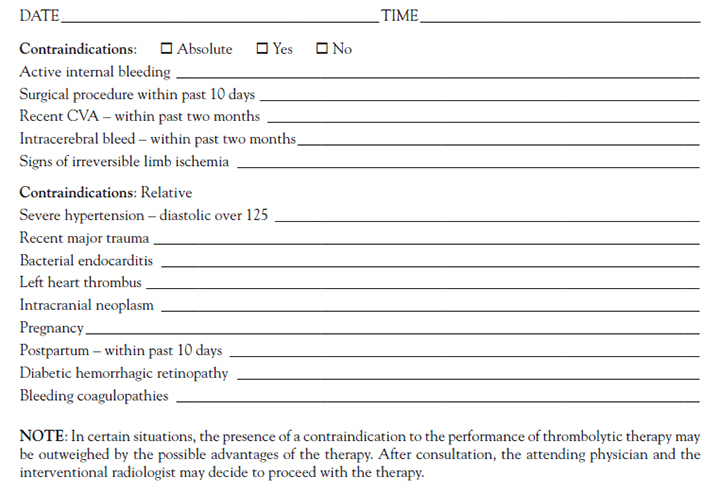
Newly formed blood clots are more susceptible to lysis, and as noted, there is some evidence that clots or emboli less than three to six hours old are more likely to dissolve with directed infusion than older lesions. Therefore, patients who present with sudden onset of pain and coolness in an extremity may be candidates for thrombolytic therapy.
Patients receiving intra-arterial thrombolytic therapy should be in an intensive care unit. Blood work should be monitored closely, with specific attention to the CBC, PT/INR, PTT, and fibrinogen levels. It is imperative to note any signs of systemic bleeding, such as hypotension and confusion. Extreme care should be taken with the arterial line. The catheter should remain taped securely in place. The drug infuses at the exact clot location, so the catheter should never be allowed to move.
Intramuscular injections or other procedures that may induce bleeding should be avoided during thrombolytic therapy administration. The drug is delivered by means of an infusion pump, and during the time of administration, patients should be continuously assessed for any signs of bleeding. The drug may be infused for six hours or longer, during which time the patient may be taken to the interventional radiology department for serial angiograms to assess the status of the dissolving clot. When the catheter is removed, special attention should be given to the puncture site and extra time for holding pressure on the site should be allowed.
With successful thrombolytic therapy, patients may be spared surgical procedures and prolonged hospitalization. Blocked arteries in the lower extremities, occluded surgical bypass grafts, dialysis access grafts, central venous occlusion, and acute upper extremity ischemia all have been helped by this form of therapy.
The superior and inferior mesenteric arteries supply blood to the small and large intestines. A disruption in blood supply in either of these arteries can lead to a variety of symptoms, including severe pain, nausea, vomiting, and diarrhea. The resulting acute mesenteric ischemia has a very high mortality rate. In certain patients, intense mesenteric vasoconstriction may occur without an obvious lesion. These are the patients who may develop mesenteric ischemia or infarction without vascular occlusion. In other words, the vessels are not obstructed by strictures or blood clots; they simply remain constricted. In cases such as these, the intra-arterial administration of papaverine hydrochloride may be lifesaving.
Papaverine, a hydrochloride of an opium alkaloid, relaxes various smooth muscles, especially those of the larger arteries. This relaxation may be pronounced, especially if spasm exists. Relaxation is noted in the vascular system and bronchial musculature and in the gastrointestinal, biliary, and urinary tracts. The antispasmodic effect is direct and is unrelated to muscle innervation.
The indication for papaverine hydrochloride therapy is confirmed at the time of the diagnostic angiogram as many other conditions can mimic these symptoms. Patients who experience acute mesenteric ischemia are quite ill and may already be receiving moderately high doses of analgesics for intense abdominal pain; consequently, IV moderate sedation for the angiogram may not be needed. In some cases, a test injection of tolazoline hydrochloride will be given directly into the affected artery to test for vasodilation activity. If the response is good, the decision may be made to institute papaverine therapy.
Papaverine hydrochloride is given via continuous pump infusion directly into the involved artery. It has an explicit relaxant effect on smooth muscle, particularly muscles in spasm. The half-life of papaverine hydrochloride is 30 minutes to two hours, so patients receiving this drug should be watched very carefully [20]. They should be taken directly from the interventional radiology suite to the intensive care unit, where the staff should be certain that the catheter is not moved from its predetermined secured site.
The most important side effect of papaverine is hypotension, as the vasodilation produced by the drug may cause a significant decrease in blood pressure. A patent intravenous line is essential to provide access for fluid administration. The only direct contraindication for papaverine is heart block, which can further increase conduction delays. The drug also should be used with extreme caution in patients with acute angle glaucoma. Abdominal pain and diarrhea during mesenteric infusion are common and may reflect successful reperfusion rather than the development of bowel infarction [20].
According to the American College of Radiology, the use of a microcatheter allows for distal access and superselective embolization of single vasa recta at the site of bleeding. Instead of embolic material, vasopressin infusion is indicated when a diffuse source of bleeding is identified or when superselective catheterization fails or is not technically possible.
(https://acsearch.acr.org/docs/69457/Narrative Last Accessed: June 1, 2022)Level of Evidence: Expert Opinion/Consensus Statement
Vasopressin causes contraction of the smooth muscle of the gastrointestinal tract. Vasopressin injection has been administered IV or intra-arterially into the superior mesenteric artery as an adjunct in the treatment of acute, massive gastrointestinal hemorrhage caused by ruptured esophageal varices, peptic ulcer disease, esophagogastritis, esophageal laceration, acute gastritis, colitis associated with Behçet syndrome, small intestinal typhoid infection, Mallory-Weiss syndrome, or intestinal perforation. Use of vasopressin in such situations is a temporary measure, intended to decrease portal venous pressure and increase clotting and hemostasis. With the advent of super-selective embolization, vasopressin is reserved for cases in which embolization would result in excessive occlusion [157].
Emergency colon surgery can be risky, and the administration of this drug can stop bleeding permanently or delay future episodes of hemorrhage until the patient is stable enough to undergo elective surgery. Once a bleeding point is established by angiographic examination, the infusion catheter is positioned in either the superior or inferior mesenteric artery and drug administration is begun by means of an infusion pump. Dosages may be titrated accordingly to control the bleeding.
Vasopressin should be used with extreme caution in patients with coronary artery disease because the vasoconstrictive effects may systematically result in constriction of the coronary arteries [20]. In such patients, even small doses may precipitate anginal pain. With larger doses, the possibility of myocardial infarction should be considered.
Vasopressin may also produce water intoxication, so early signs of drowsiness, listlessness, and headaches should be recognized to prevent serious effects [20]. The patient receiving intra-arterial vasopressin should be in an intensive care unit where any signs of angina may be observed. The staff should carefully monitor urinary output and observe for abdominal cramping and change in stool color.
Vasopressin should never be stopped suddenly. It is extremely important to taper the dosage when stopping intra-arterial administration of the drug.
Naturally, when contemplating any medical procedure, the welfare of the patient and involved staff should be evaluated. This applies to all facets of interventional radiology, but the use of ionizing radiation in x-ray, CT, radiation therapy, and nuclear medicine procedures is of particular concern.
Medical radiation exposure now accounts for the largest man-made source of ionizing radiation [158]. In order to minimize the radiation dose to the staff, individual patient, and society as a whole, radiation levels should be kept as low as possible. The concept of "as low as reasonably achievable" (ALARA) was developed to help provide a sound safety principle. It is now a federal regulatory requirement for all radiation safety programs [159]. Basically, ALARA is a common sense approach to the allowable radiation doses received by individuals, but it also includes guidelines that should be followed to achieve these levels.
CT and fluoroscopy provide some of the largest radiation doses among the more common interventional radiology procedures. Using ultrasound or another nonionizing radiation imaging technique could help reduce the radiation dose administered to each patient. When possible, follow-up imaging with ultrasound or MRI, instead of CT, would also help. Unfortunately, MRI remains more expensive than other imaging modalities.
The guidelines for general safety prepared by the American College of Radiology and SIR have been mentioned in this course. These guidelines include a list of things to consider before, during, and after an interventional radiology procedure. Simple items, such as not implanting nickel-titanium alloy stents or filters into patients with nickel allergies or being certain that the patient is well grounded prior to administering radiofrequency ablation, can prevent unwanted consequences.
Interventional radiology is primarily concerned with treating existing morbidities, with the main exception of angiography, and adverse effects of guided imaging are generally considered acceptable risks because they are comparably less important than life-saving procedures or vast improvements in quality of life. Nonetheless, it should be remembered that the ALARA protocol recognizes that no level of radiation is known to be completely safe, and a conscious effort should be made by all healthcare professionals to use diagnostic and follow-up imaging sparingly [159].
In 2020, CT scans were performed at the rate of more than 220 per 1,000 Americans [160]. It has been estimated that in the next few decades nearly 30,000 cancers will be caused by exposure to this radiation. Others feel this is an overestimate and that the risk of cancer is actually reduced by having CT scans (at least for adults) due to a process called radiation activated natural protection, whereby small doses of intense radiation kill precancerous cells and provide immunity against future cancers [161]. In either case, imaging statistics have revealed trends of unnecessary procedures, duplicate testing, and physician self-referral, causing more than $26 billion in excess healthcare expenditures and a corresponding increase in health insurance cost [162,163]. There are many factors that may be contributing to these trends, including the increase in available technology and physicians trained to use it, a rise in the practice of defensive medicine, and the use of physician-induced care. However, the fact remains that millions of radiologic tests will be performed each year, of which 20% to 50% are redundant or not beneficial to patients' diagnosis and treatment [164,165]. Various studies have found [166,167,168,169,170]:
Americans were exposed to seven times more medical radiation in 2006 than in the early 1980s, mostly due to increased usage of CT scans.
One in five hospital imaging tests are duplicates, possibly due to a lack of ready access to medical records or transfers to a different facility.
Self-referring physicians are almost eight times as likely to order imaging compared with non-self-referring physicians, with significantly higher costs.
An estimated 14% of nuclear cardiac stress tests are not appropriate, according to the American College of Cardiology criteria. Each test is equivalent to 500 to 1,000 chest x-rays and costs roughly $2,000.
About 62% of elective coronary catheterizations are unfounded.
From a purely economic standpoint, this kind of waste can be considered a moral hazard. In many cases, the negative repercussions of imaging overuse are passed on to the patient, while the facility and physicians experience no downside. Additionally, ordering many tests is considered by some to be an effective risk management strategy. However, there is a substantial gap between physicians' perceived risk of malpractice and their actual risk, with physicians perceiving a much greater risk of malpractice than has been documented for their specialty [171,172]. For example, in a survey of neurologists, respondents estimated that 8 per 100 neurologists in their state would be sued within the following year; this compared with American Medical Association data that indicated a risk of 1.49 per 100 [173,174]. Similarly, radiologists have estimated their risk of litigation within five years as 35%, which compares with an actual rate of approximately 10% [171].
Balancing the benefits and risks to patients, the risks of litigation, and, possibly, the burden on the healthcare system can be challenging. It is important to reflect on this balance from time to time in order to ensure that patients continue to receive safe and effective care.
While the vast majority of patients who undergo short-stay radiologic procedures do very well, complications can and do occur. It is important to always discuss the possible complications when explaining procedures to patients before the informed consent form is completed. A nurse can serve as a resource person to clarify and reinforce key points and help assess how well the patient and family members comprehend the upcoming procedure and its possible and anticipated outcomes.
Communication with patients regarding interventional procedures and expectations is a vital aspect of promoting positive outcomes. An interpreter should be acquired if the patient is more comfortable communicating in another language. Frequently, this may be easier said than done, as there may be institutional and/or patient barriers. In the multicultural landscape, interpreters are a valuable resource to help bridge the communication and cultural gaps between patients and practitioners. Interpreters are more than passive agents who translate and transmit information back and forth from party to party. When they are enlisted and treated as part of the interdisciplinary clinical team, interpreters serve as cultural brokers, who ultimately enhance the clinical encounter. When providing care for patients for whom English is a second language, the presentation of education materials in the individual's native language may improve understanding and outcomes.
It is during instruction that patients usually hear that the benefits of the procedure greatly outweigh any possible risks. In certain instances, however, risks become greater, and in those cases, patients and their families should be aware of what sequelae could result. All these procedures are, by definition, invasive, and invasive procedures interfere with the natural defenses of the body.
In some hospitals and imaging centers, signed consent is obtained before patients receive intravenous x-ray dye for a basic CT scan or dye injection. Whether this protocol is in effect, it is important that patients understand why the contrast is being given, how it works, and what feelings and sensations they may experience during its administration. Contrast materials are usually given by a power injector, with a bolus injection of up to 150 cc into the vein at a flow rate of 2–4 cc per second.
CT contrast materials usually have an iodine base, but even nonionic agents have a potential for reactions. The nonionic dyes are less likely to cause electrical interference in the heart, cerebral symptoms, hives, itching, nausea, or vomiting. However, patients still have the potential to respond adversely as the dye rapidly mixes with the circulating blood volume. Mild reactions are not unusual. Many patients experience a warm or hot flush or a metallic taste that disappears within one to two minutes. Hopefully, any patient who has previously reacted to iodinated contrast medium should know about this reaction.
As with any allergy, a person should be aware that this drug may present a potentially life-threatening problem in the future. Convulsions, pulmonary edema, hypotensive shock, and cardiorespiratory arrest are possible life-threatening reactions. It is vital to advise the person who has a reaction that he or she is allergic to the contrast medium and inform other healthcare personnel of this should any future studies requiring contrast agents be considered. In this way, the pros and cons of contrast administration may be properly evaluated. Premedication may be necessary or contrast materials may need to be totally withheld. An MRI, ultrasound, or nuclear medicine examination may offer similar yet safer results for a patient who has had an allergic reaction to a contrast agent in the past.
It should be noted that the radiology staff has a responsibility to communicate with all of the patient's caregivers if a patient has a problem with the contrast medium. A complete report should be given so that the floor or short-stay staff is aware of the reason the patient returns with hives or comes back sleepy from a diphenhydramine injection.
IV moderate sedation is another area that the staff may take for granted. Although there are a few patients who ask to be awake so that they can watch the procedures on the video screen, most patients prefer to sleep through the procedure. It is important to make patients and their family members aware that IV moderate sedation is not general anesthesia and it is given to relax the patient just enough to assure that he or she is as comfortable as possible. Staff members who are familiar with moderate sedation often hear patients tell them that they are still awake and need more medicine to go to sleep. Patient teaching should include the fact that small doses are given as needed and patients do not have to be sound asleep for these types of procedures. In fact, many procedures require that patients cooperate with breath holding and not moving a certain body part.
It is possible that the respiratory depressant effects of moderate sedation may last longer in certain patients, which is one reason that patients should be closely observed in the same-day surgical area or on the medical-surgical floor for several hours. The radiology staff's responsibility for teaching extends to all members of the medical staff who will be in contact with these patients during the postprocedure hours. Respiratory depression, hypotension, nausea, and vomiting are serious potential side effects from the use of IV moderate sedation.
Before patients are discharged, they should be assessed for stability of vital signs, return of all reflexes, satisfactory airway, complete motor control, and alertness or a return to the preprocedure level of consciousness. Instructions should be both verbal and written and should stress the importance of avoiding alcohol intake, driving, or operating heavy machinery until the following day.
All procedures present some degree of risk. Unlike open surgery, in which an organ or tissue is sampled directly, interventional radiologic procedures use guidance systems to provide indirect visualization of the organ systems. With conventional surgery, bleeding sites and perforations may be plainly noted, but this is not the case with transcutaneous procedures. Complications do happen, and patients, families, and healthcare workers should be aware of their potential.
All those involved should be aware of the normal reactions and what may be indicative of more serious problems. Any time a puncture is made into living tissue, there is some bleeding to be expected. That is the basic reason that direct pressure is applied to a venipuncture site. When a puncture is made or a piece of tissue is sampled by means of a long needle, however, no such direct pressure can be exerted. Therefore, it is normal for some bleeding to occur, and that concept should be made clear. The trick is to be able to discern when there is a real problem.
Any blood, even just a few drops, that leaks onto the peritoneum causes irritation and pain. If the site is near the diaphragm, the blood may cause irritation to the diaphragm or phrenic nerve and the patient may have some referred shoulder pain, hiccoughing, or pain with deep breathing. All pain, however, is subjective, and what one patient may consider to be excruciating, another may barely notice. This is why all patients should be observed closely for classic signs of hemorrhage and dyspnea for several hours before they are sent home. The written instructions should be reinforced at this time by the discharging nurse, who should be certain that patients and their caregiver(s) know what to do if they feel there is an exacerbation in or new onset of any postoperative symptoms.Table 9 is an example of an instruction form that can be sent home with the patient.
Certain procedures carry their own risks. A lung biopsy patient should be made aware of the importance of calling for assistance if he or she should experience sudden difficulty breathing. This is not to be compared to soreness at the surgical site or the immediate postprocedure discomfort with deep breathing.
Patients who have undergone pancreatic or hepatic procedures have a slight but real chance of developing pancreatitis or a small bile leak. These patients should be informed that fever, vomiting, chills, and increased pain are danger signs that may indicate an acute abdomen. This is a complication that may result from any abdominal procedure, including celiac plexus blocks, transhepatic cholangiograms, cyst drainages, TIPS, and various biopsy procedures.
Angiography and angioplasty patients should be fully aware of the real potential for postprocedure bleeding. While some facilities use sandbags over arterial puncture sites, others do not. There is a possibility that if the femoral artery leaks, it can quickly pump quite a bit of blood into the compressing sandbag before the hemorrhage is discovered. Patients and short-stay procedure staff should be told of the importance of keeping the leg straight and relatively immobile for several hours after the procedure. It is not at all rare for a site to begin bleeding again when motion or ambulation is started too early. Before discharge, the written instructions should be verbally reinforced, along with a demonstration of how to apply pressure if bleeding does occur. Most angiography patients experience some type of ecchymosis or even a small hematoma at their puncture sites. Education should include the signs of significant bleeding into the tissue around the groin, as some hemorrhages can be internal rather than overt.
A cool leg with a change in color may signify a problem with a blood clot. Pain, the most common sign of embolus, is obvious to the patient, but all involved should be taught the importance of direct visualization of both extremities after an angiogram or angioplasty. Both staff and caregivers should remember that most often a puncture in the right side of the groin means that the repair of the vessel has been performed on the opposite side. Therefore, pain and discoloration of the left leg should not be ignored simply because the puncture is on the right side.
A swollen arm after a subclavian stent insertion should not be taken lightly. Strictures may form and clots may develop in and around these areas, which lead to compromised circulation. Patients should be aware that an arm that gradually increases in size may signal a significant problem.
The importance of educating patients, home caregivers, and staff cannot be overstressed. While the benefits of short-stay procedures overwhelmingly surpass older techniques of open surgery with corresponding long hospitalizations, it is necessary to anticipate the complications that may occur. Simply saying that problems may happen is not enough. Nurses' role as teachers should be realized, and education of patients and staff should be a high priority.
All fields of medicine are continually improving and becoming more complex, and interventional radiology remains one of the most rapidly expanding specialties. New procedures, techniques, and equipment improvements occur on a frequent basis, and it can be difficult to keep up with all of the changes.
This course has attempted to present the status of some of the more common interventional radiology procedures and to place them into the framework of the typical radiology department. Obviously, not all interventional radiology procedures could be discussed, and all of the techniques, procedures, and available technology are subject to change. Therefore, the reader is encouraged to consult the latest literature on the subject.
1. Mould RF. The early history of x-ray diagnosis with emphasis on the contributions of physics 1895–1915. Phys Med Biol. 1995;40(11):1741-1787.
2. U.S. Food and Drug Administration. Radiation-Emitting Products: Fluoroscopy. Available at https://www.fda.gov/radiation-emitting-products/medical-x-ray-imaging/fluoroscopy. Last accessed May 12, 2022.
3. Mayo Clinic. CT Scan: Overview. Available at https://www.mayoclinic.org/tests-procedures/ct-scan/about/pac-20393675. Last accessed May 12, 2022.
4. Mayo Clinic. MRI: Overview. Available at https://www.mayoclinic.org/tests-procedures/mri/about/pac-20384768. Last accessed May 12, 2022.
5. U.S. Food and Drug Administration. [Archive]. Public Health Advisory: Gadolinium-Containing Contrast Agents for Magnetic Resonance Imaging (MRI). Available at https://wayback.archive-it.org/7993/20170406045321/https://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm053112.htm. Last accessed May 12, 2022.
6. U.S. Food and Drug Administration. [Archive]. Information for Healthcare Professionals: Gadolinium-Containing Contrast Agents for Magnetic Resonance Imaging (MRI) (Marketed as Omniscan, OptiMARK, Magnevist, ProHance, and MultiHance). Available at https://wayback.archive-it.org/7993/20170722191207/https://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm142911.htm. Last accessed May 12, 2022.
7. U.S. Food and Drug Administration. [Archive]. Questions and Answers on Gadolinium-Based Contrast Agents. Available at https://wayback.archive-it.org/7993/20170406045310/https://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm142889.htm. Last accessed May 12, 2022.
8. U.S. Food and Drug Administration. FDA Drug Safety Communication: FDA Evaluating the Risk of Brain Deposits with Repeated Use of Gadolinium-Based Contrast Agents for Magnetic Resonance Imaging (MRI). Available at https://www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-communication-fda-evaluating-risk-brain-deposits-repeated-use-gadolinium-based. Last accessed May 12, 2022.
9. U.S. Food and Drug Administration. [Archive]. Radiation-Emitting Products: Ultrasound Imaging. Available at https://wayback.archive-it.org/7993/20171101110117/https://www.fda.gov/Radiation-EmittingProducts/RadiationEmittingProductsandProcedures/MedicalImaging/ucm115357.htm. Last accessed May 12, 2022.
10. U.S. Food and Drug Administration. FDA Drug Safety Communication: New Warnings for Using Gadolinium-Based Contrast Agents in Patients with Kidney Dysfunction. Available at https://www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-communication-new-warnings-using-gadolinium-based-contrast-agents-patients-kidney. Last accessed May 12, 2022.
11. U.S. Food and Drug Administration. FDA Drug Safety Communication: FDA Warns That Gadolinium-Based Contrast Agents (GBCAs) Are Retained in the Body; Requires New Class Warnings. Available at https://www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-communication-fda-warns-gadolinium-based-contrast-agents-gbcas-are-retained-body. Last accessed May 12, 2022.
12. U.S. Food and Drug Administration. FDA Drug Safety Communication: FDA Identifies No Harmful Effects to Date with Brain Retention of Gadolinium-Based Contrast Agents for MRIs; Review to Continue. Available at https://www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-communication-fda-identifies-no-harmful-effects-date-brain-retention-gadolinium. Last accessed May 12, 2022.
13. Campbell JD, Elford RW, Brant RF. Case-control study of prenatal ultrasonography exposure in children with delayed speech. CMAJ. 1993;149(10):1435-1440.
14. Salvesen KA. EFSUMB: safety tutorial: epidemiology of diagnostic ultrasound exposure during pregnancy-European committee for medical ultrasound safety (ECMUS). Eur J Ultrasound. 2002;15(3):165-171.
15. Newnham JP, Doherty DA, Kendall GE, Zubrick SR, Landau LL, Stanley FJ. Effects of repeated prenatal ultrasound examinations on childhood outcome up to 8 years of age: follow-up of a randomized controlled trial. Lancet. 2004;364(9450):2038-2044.
16. U.S. Food and Drug Administration. Avoid Fetal "Keepsake" Images, Heartbeat Monitors. Available at https://www.fda.gov/consumers/consumer-updates/avoid-fetal-keepsake-images-heartbeat-monitors. Last accessed May 12, 2022.
18. Vallabhajosula S. Positron emission tomography radiopharmaceuticals for imaging brain Beta-amyloid. Semin Nucl Med. 2011;41(4):283-299.
19. Society of Interventional Radiology. What is Interventional Radiology? Available at https://www.sirweb.org/patient-center/conditions-and-treatments/what-is-interventional-radiology. Last accessed May 12, 2022.
20. Lexicomp Online. Available at https://online.lexi.com. Last accessed May 12, 2022.
21. Daley BJ, Taylor D, Goicolea JFA. Perioperative Anticoagulation Management. Available at https://emedicine.medscape.com/article/285265-overview. Last accessed May 12, 2022.
22. Mahnken AH, Wilhelm KE, Ricke J (eds). CT- and MR-Guided Interventions in Radiology. 2nd ed. Berlin: Springer; 2013.
23. Siddiqi NH. Contrast Medium Reactions. Available at https://emedicine.medscape.com/article/422855-overview. Last accessed May 12, 2022.
24. Maddox TG. Adverse reactions to contrast material: recognition, prevention, and treatment. Am Fam Physician. 2002;66(7):1229-1235.
25. Hunt CH, Hartman RP, Hesley GK. Frequency and severity of adverse effects of iodinated and gadolinium contrast materials: retrospective review of 456,930 doses. Am J Roentgenol. 2009;193(4):1124-1127.
26. Lasser EC, Berry CC, Talner LB, et al. Pretreatment with corticosteroids to alleviate reactions to intravenous contrast material.N Engl J Med. 1987;317(14):845-849.
27. Barkin JS, Casal GL, Reiner DK, Goldberg RI, Phillips RS, Kaplan S. A comparative study of contrast agents for endoscopic retrograde pancreatography. Am J Gastroenterol. 1991;86(10):1437-1441.
28. Juels AN, Windle ML. Procedural Sedation. Available at https://emedicine.medscape.com/article/109695-overview. Last accessed May 12, 2022.
29. The Joint Commission. Comprehensive Accreditation Manual for Hospitals: The Official Handbook. Oakbrook Terrace, IL: Joint Commission Resources; 2018.
30. The Joint Commission. Standards FAQs: Hospital and Hospital Clinics: Provision of Care, Treatment, and Services (PC): Sedation and Anesthesia: Understanding the Assessment Requirements. Available at https://www.jointcommission.org/standards/standard-faqs/hospital-and-hospital-clinics/provision-of-care-treatment-and-services-pc/000001645/. Last accessed May 12, 2022.
31. American Society of Anesthesiologists. ASA Physical Status Classification System. Available at https://www.asahq.org/resources/clinical-information/asa-physical-status-classification-system. Last accessed May 12, 2022.
33. Aldrete JA. Modifications to the postanesthesia score for use in ambulatory surgery. J Perianesth Nurs. 1998;13(3):148-155.
35. Olkkola KT, Ahonen J. Midazolam and other benzodiazepines. Handb Ex Pharmacol. 2008;(182):335-360.
36. Society of Interventional Radiology. Patient Center: Glossary of Interventional Radiology Treatments. Available at https://www.sirweb.org/patient-center/conditions-and-treatments/glossary-of-ir-treatments. Last accessed May 12, 2022.
37. Society of Interventional Radiology. ACR-SIR-SPR Practice Parameter for the Performance of Image-Guided Percutaneous Needle Biopsy (PNB). Available at https://www.acr.org/-/media/ACR/Files/Practice-Parameters/PNB.pdf. Last accessed May 12, 2022.
38. Vilmann P, Larsen SS. Endoscopic ultrasound-guided biopsy in the chest: little to lose, much to gain. Eur Respir J. 2005;25(3):400-401.
39. Boskovic T, Stanic J, Pena-Karan S, et al. Pneumothorax after transthoracic needle biopsy of lung lesions under CT guidance.J Thorac Dis. 2014;6(Suppl 1):S99-S107.
40. Cholongitas E, Quaglia A, Samonakis D, et al. Transjugular liver biopsy: how good is it for histological interpretation? Gut. 2006;55(12):1789-1794.
41. Tan KT, Rajan DK, Kachura JR, Hayeems E, Simons ME, Ho CS. Pain after percutaneous liver biopsy for diffuse hepatic disease: a randomized trail comparing subcostal and intercostal approaches. J Vasc Interv Radiol. 2005;16(9):1215-1219.
42. Strobel D, Bernatik T, Blank W, et al. Incidence of bleeding in 8172 percutaneous ultrasound-guided intraabdominal diagnostic and therapeutic interventions—results of the prospective multicenter DEGUM interventional ultrasound study (PIUS study). Ultraschall Med. 2015;36(2):122-131.
43. Bihl GR, Petri M, Fine DM. Kidney biopsy in lupus nephritis: look before you leap. Nephrol Dial Transplant. 2006;21(7):1749-1752.
44. Brent LW. Lupus Nephritis Workup: Kidney Biopsy. Available at https://emedicine.medscape.com/article/330369-workup#c9. Last accessed May 12, 2022.
45. Blake MA, Sweeney AT. Pheochromocytoma. Available at https://emedicine.medscape.com/article/124059-overview. Last accessed May 12, 2022.
46. Ahrar K, Himmerich JU, Herzog CE, et al. Percutaneous ultrasound-guided biopsy in the definitive diagnosis of osteosarcoma.J Vasc Interv Radiol. 2004;15(11):1329-1333.
47. Yu SC. The utility of a drainage needle for percutaneous abscess drainage. Am J Roentgenol. 2005;185(1):58-63.
48. Rosenberg S, Courtney A, Nemeck AA Jr, Omary RA. Comparison of percutaneous management techniques for recurrent malignant ascites. J Vasc Interv Radiol. 2004;15(10):1129-1131.
49. Caldwell J, Edriss H, Nugent K. Chronic peritoneal indwelling catheters for the management of malignant and nonmalignant ascites. Proc (Bayl Univ Med Cent). 2018;31(3):297-302.
50. Jaffe TA, Nelson RC, DeLong DM, Paulson EK. Practice patterns in percutaneous image-guided intra-abdominal abscess drainage: survey of academic and private centers. Radiology. 2004;233(3):750-756.
51. Gervais DA, Ho CH, O'Neill MJ, Arellano RS, Hahn PF, Mueller PR. Recurrent abdominal and pelvic abscesses: incidence, results of repeated percutaneous drainage, and underlying causes in 956 drainages. Am J Roentgenol. 2004;182(2):463-466.
52. de Groof EJ, Carbonnel F, Buskens CJ, Bemelman WA. Abdominal abscess in Crohn's disease: multidisciplinary management.Dig Dis. 2014;32(Suppl 1):103-109.
53. Schildhouse R, Lai A, Barsuk JH, Mourad M, Chopra V. Safe and effective bedside thoracentesis: a review of the evidence for practicing clinicians. J Hosp Med. 2017;12(4):266-276.
54. Redden MD, Chin TY, van Driel ML. Surgical versus non-surgical management for pleural empyema. Cochrane Database Syst Rev. 2017;3:CD010651.
55. Visser BC, Muthusamy VR, Yeh BM, Coakley FV, Way LW. Diagnostic evaluation of cystic pancreatic lesions. HPB (Oxford). 2008;10(1):63-69.
56. Pelaez-Luna M, Chari ST. Cyst fluid analysis to diagnose pancreatic cystic lesions: an as yet unfulfilled promise. Gastroenterology. 2006;130(3):1007-1009.
57. Lopes CV. Cyst fluid glucose: an alternative to carcinoembryonic antigen for pancreatic mucinous cysts. World J Gastroenterol. 2019;25(19):2271-2278.
58. Faias S, Pereira L, Roque R, et al. Excellent accuracy of glucose level in cystic fluid for diagnosis of pancreatic mucinous cysts.Dig Dis Sci. 2020;65(7):2071-2078.
59. Jabbar KS, Verbeke C, Hyltander AG, Sjövall H, Hansson GC, Sadik R. Proteomic mucin profiling for the identification of cystic precursors of pancreatic cancer. J Natl Cancer Inst. 2014;106(2):djt439.
60. Moutinho-Ribeiro P, Macedo G, Melo SA. Pancreatic cancer diagnosis and management: has the time come to prick the bubble? Front Endocrinol (Lausanne). 2019;9:779.
61. Morris-Stiff G, Lentz G, Chalikonda S, et al. pancreatic cyst aspiration analysis for cystic neoplasms: mucin or carcinoembryonic antigen—which is better? Surgery. 2010;148(4):638-644.
62. Utomo WK, Braat H, Bruno MJ, et al. Cytopathological analysis of cyst fluid enhances diagnostic accuracy of mucinous pancreatic cystic neoplasms. Medicine (Baltimore). 2015;94(24):e988.
63. Kariniemi J, Sequeiros RB, Ojala R, Tervonen O. Feasibility of MR imaging-guided percutaneous drainage of pancreatic fluid collections. J Vasc Interv Radiol. 2006;17(8):1321-1326.
64. Wybranski C, Strach K, Krenzien F, et al. Percutaneous abscess drainage using near real-time MR guidance in an open 1.0-T MR scanner: proof of concept. Invest Radiol. 2013;48(6):477-484.
65. Zerem E, Hauser G, Loga-Zec S, Kunosić S, Jovanović P, Crnkić D. Minimally invasive treatment of pancreatic pseudocysts.World J Gastroenterol. 2015;21(22):6850-6860.
66. Aboumarzouk OM, Kata SG, Keeley FX, McCliton S, Nabi G. Extracorporeal shock wave lithotripsy (ESWL) versus ureteroscopic management for ureteric calculi. Cochrane Database Syst Rev. 2012;5:CD006029.
67. Siddiqi NH. Percutaneous Nephrostomy. Available at https://emedicine.medscape.com/article/1821504-overview. Last accessed May 12, 2022.
68. Srisubat A, Potisat S, Lojanapiwat B, Setthawong V, Laopaiboon M. Extracorporeal shock wave lithotripsy (ESWL) versus percutaneous nephrolithotomy (PCNL) or retrograde intrarenal surgery (RIRS) for kidney stones. Cochrane Database Syst Rev. 2014;11:CD007044.
69. Dyer RB, Regan JD, Kavanagh PV, Khatod EG, Chen MY, Zagoria RJ. Percutaneous nephrostomy with extensions of the technique: step by step. Radiographics. 2002;22(3):503-525.
70. Al-Aown A, Kyriazis I, Kallidonis P. Ureteral stents: new ideas, new designs. Ther Adv Urol. 2010;2(2):85-92.
71. Song HY, Park H, Suh TS, et al. Recurrent traumatic urethral strictures near the external sphincter: treatment with covered, retrievable, expandable nitinol stent—initial results. Radiology. 2003;226(2):433-440.
72. Dawood A, Jayaraman V. Percutaneous Cholangiography. Available at https://emedicine.medscape.com/article/1828033-overview. Last accessed May 12, 2022.
73. Ignee A, Cui X, Schuessler G, Dietrich CF. Percutaneous transhepatic cholangiography and drainage using extravascular contrast enhanced ultrasound. Z Gastroenterol. 2015;53(5):385-390.
74. Nolsøe CP, Nolsøe AB, Klubien J, et al. Use of ultrasound contrast agents in relation to percutaneous interventional procedures: a systematic review and pictorial essay. J Ultrasound Med. 2018;37(6):1305-1324.
75. Johnson PL. Biliary Stenting. Available at https://emedicine.medscape.com/article/1828072-overview. Last accessed May 12, 2022.
76. Burke DR, Lewis CA, Cardella JF, et al. Quality improvement guidelines for percutaneous transhepatic cholangiography and biliary drainage. J Vasc Interv Radiol. 2003;14(9 Pt 2);S243-S246.
78. Applegate RJ, Sacrinty MT, Kutcher MA, et al. Trends in vascular complications after diagnostic cardiac catheterization and percutaneous coronary intervention via the femoral artery, 1998 to 2007. JACC Cardiovasc Interv. 2008;1(3):317-326.
79. Nathan S, Rao SV. Radial versus femoral access for percutaneous coronary intervention: implications for vascular complications and bleeding. Curr Cardiol Rep. 2012;14(4):502-509.
80. Mamas MA, Ratib K, Routledge H, et al. Influence of arterial access site selection on outcomes in primary percutaneous coronary intervention: are the results of randomized trials achievable in clinical practice? JACC Cardiovasc Interv. 2013;6(7):698-706.
82. Machecourt J, Bonnefoy E, Vanzetto G, et al. Primary angioplasty is cost-minimizing compared with pre-hospital thrombolysis for patients within 60 min of a percutaneous coronary intervention center: the Comparison of Angioplasty and Pre-hospital Thrombolysis in Acute Myocardial Infarction (CAPTIM) cost-efficacy sub-study. J Am Coll Cardiol. 2005;45(4):515-524.
83. Bittl JA, Chew DP, Topol EJ, Kong DF, Califf RM. Meta-analysis of randomized trials of percutaneous transluminal coronary angioplasty versus atherectomy, cutting balloon atherotomy, or laser angioplasty. J Am Coll Cardiol. 2004;43(6):936-942.
84. Fernández-Avilés F, Alonso JJ, Peña G, et al. Primary angioplasty vs. early routine post-fibrinolysis angioplasty for acute myocardial infarction with ST-segment elevation: the GRACIA-2 non-inferiority, randomized, controlled trail. Eur Heart J. 2007;28(8):949-960.
85. Pentecost MJ, Criqui MH, Dorros G, et al. Guidelines for peripheral percutaneous transluminal angioplasty of the abdominal aorta and lower extremity vessels. A statement for health professionals from a Special Writing Group of the Councils on Cardiovascular Radiology, Arteriosclerosis, Cardio-Thoracic and Vascular Surgery, Clinical Cardiology, and Epidemiology and Prevention, the American Heart Association. J Vasc Interv Radiol. 2003;14(9 Pt 2):S495-S515.
86. Bountouris I, Kristmundsson T, Dias N, Zdanowski Z, Malina M. Is repeat PTA of a failing hemodialysis fistula durable? Int J Vasc Med. 2014:369687.
87. Miquelin DG, Reis LF, da Silva AA, de Godoy JM. Percutaneous transluminal angioplasty in the treatment of stenosis of arteriovenous fistulae for hemodialysis. Int Arch Med. 2008;1(1):16.
88. Buccheri D, Piraino D, Andolina G, Cortese B. Understanding and managing in-stent restenosis: a review of clinical data, from pathogenesis to treatment. J Thorac Dis. 2016;8(10):E1150-E1162.
89. Dibra A, Kastrati A, Alfonso F, et al. Effectiveness of drug-eluting stents in patients with bare-metal in-stent restenosis: a meta-analysis of randomized trials. J Am Coll Cardiol. 2007;49(5):616-623.
90. Alfonso F, Pérez-Vizcayno MJ, Hernandez R, et al. A randomized comparison of sirolimus-eluting stent with balloon angioplasty in patients with in-stent restenosis: results of the Restenosis Intrastent: Balloon Angioplasty Versus Elective Sirolimus-Eluting Stenting (RIBS-II) trial. J Am Coll Cardiol. 2006;47(11):2152-2160.
91. Holmes DR Jr, Teirstein P, Satler L, et al. Sirolimus-eluting stents vs. vascular brachytherapy for in-stent restenosis within bare-metal stents: the SISR randomized trial. JAMA. 2006;295(11):1264-1273.
92. Mukherjee D, Moliterno DJ. Brachytherapy for in-stent restenosis: a distant second choice to drug-eluting stent placement. JAMA. 2006;295(11):1307-1309.
93. Alfonso F, Perez-Vizcayno MJ, Hernandez R, et al. Long-term clinical benefit of sirolimus-eluting stents in patients with in-stent restenosis results of the RIBS-II (Restenosis Intra-stent: Balloon angioplasty vs elective sirolimus-eluting Stenting) study. J Am Coll Cardiol. 2008;52(20):1621-1627.
94. Waksman R, Iantorno M. Refractory in-stent restenosis: improving outcomes by standardizing our approach. Curr Cardiol Rep. 2018;20(12):140.
95. U.S. Food and Drug Administration. Premarket Approval: BARD E-LUMINEXX Vascular Stent: Labeling. Available at https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpma/pma.cfm?id=P080007. Last accessed May 12, 2022.
96. U.S. Food and Drug Administration. LifeStent FlexStar XL Vascular Stent: P070014. Available at https://www.accessdata.fda.gov/cdrh_docs/pdf7/P070014a.pdf. Last accessed May 12, 2022.
97. Rogers FB, Mark D, Velmahos G, Rozycki G, Luchette F. Venous thromboembolism: role of vena cava filter in the prophylaxis and treatment of PE. J Trauma. 2002;53(1):142-164.
98. Velmahos GC, Kern J, Chan LS, Oder D, Murray JA, Shekelle P. Prevention of venous thromboembolism after injury: an evidence-based report--part II: analysis of risk factors and evaluation of the role of vena caval filters. J Trauma. 2000;49(1):140-144.
99. Siskin GP, Cho KJ. Inferior Vena Cava Filters. Available at https://emedicine.medscape.com/article/419796-overview. Last accessed May 12, 2022.
100. Kaufman JA, Kinney TB, Streiff MB, et al. Guidelines for the use of retrievable and convertible vena cava filters: report from the Society of Interventional Radiology multidisciplinary consensus conference. J Vasc Interv Radiol. 2006;17(3):449-459.
101. Stein PD, Matta F, Hugher MJ. Prophylactic inferior vena cava filters in patients with fractures of the pelvis or long bones. J Clin Orthop Trauma. 2018;9(2):175-180.
103. Endovascular Today. FDA Updates Safety Communication on IVC Filter Retrieval. Available at https://evtoday.com/2014/05/07/fda-updates-safety-communication-on-ivc-filter-retrieval. Last accessed May 12, 2022.
104. Geerts W, Selby R. Inferior vena cava filter use and patient safety: legacy or science? Hematology Am Soc Hematol Educ Program. 2017;2017(1):686-693.
105. Smith TP. Embolization in the external carotid artery. J Vasc Interv Radiol. 2006;17(12):1897-1912.
106. Dubel GJ, Ahn SH, Soares GM. Transcatheter embolization in the management of epistaxis. Semin Intervent Radiol. 2013;30(3):249-262.
107. Volkers NA, Hehenkamp WJK, Birnie E, et al. Uterine artery embolization in the treatment of symptomatic uterine fibroid tumors (EMMY trial): periprocedural results and complications. J Vasc Interv Radiol. 2006;17(3):471-480.
108. Interventional News. Unilateral UAE Effective for Unilateral Fibroid Disease with Supply from Only One Uterine Artery. Available at https://interventionalnews.com/unilateral-uae-effective-for-unilateral-fibroid-disease-with-supply-from-only-one-uterine-artery. Last accessed May 12, 2022.
109. Tropeano G, Amoroso S, Scambia G. Non-surgical management of uterine fibroids. Hum Reprod Update. 2008;14(3):259-274.
110. Gupta JK, Sinha A, Lumsden MA, Hickey M. Uterine artery embolization for symptomatic uterine fibroids. Cochrane Database Syst Rev. 2014;12:CD005073.
111. Serres-Cousine O, Kujiper FM, Curis E, Atashroo D. Clinical investigation of fertility after uterine artery embolization. Am J Obstet Gynecol. 2021;225(4):e1-e403.
112. Lavenson GS Jr. The carotid artery ultrasound report: considerations in evaluation and management. J Vascular Ultrasound. 2004;28(1):15-19.
113. Topol EJ, Yadav JS. Recognition of the importance of embolization in artherosclerotic vascular disease. Circulation. 2000;101(5):570-580.
114. Seriki DM, Ashleigh RJ, Butterfield JS, et al. Midterm follow-up of a single-center experience of endovascular repair of abdominal aortic aneurysms with use of the Talent stent-graft. J Vasc Interv Radiol. 2006;17(6):973-977.
115. D'Elia P, Tyrrell M, Azzaoui R, et al. Zenith abdominal aortic aneurysm endovascular graft: a literature review. J Cardiovasc Surg (Torino). 2009;50(2):165-170.
116. Torsello G, Osada N, Florek HJ, et al. Long-term outcome after Talent endograft implantation for aneurysms of the abdominal aorta: a multicenter retrospective study. J Vasc Surg. 2006;43(2):277-284.
117. van Keulen JW, de Vries JP, Dekker H, et al. One-year multicenter results of 100 abdominal aortic aneurysm patients treated with the Endurant stent graft. J Vasc Surg. 2011;54(3):609-615.
118. Amaoutakis DJ, Zammert M, Karthikesalingam A, Belkin M. Endovascular repair of abdominal aortic aneurysms. Best Pract Res Clin Anaesthesiol. 2016;30(3):331-340.
119. Jamieson WR. Advanced technologies for cardiac valvular replacement, transcatheter innovations and reconstructive surgery. Surg Technol Int. 2006;15:149-187.
120. Almeida CL, Chaturvedi R, Lee K-J, et al. Abstract 1932: percutaneous pulmonary valve implantation—the first North American trial. Circulation. 2006;114(18):385.
121. Nordmeyer J, Coats L, Lurz P, et al. Percutaneous pulmonary valve-in-valve implantation: a successful treatment concept for early device failure. Eur Heart J. 2008;29(6):810-815.
122. Cubeddu RJ, Palacios IF. Percutaneous heart valve replacement and repair: advances and future potential. Expert Rev Cardiovasc Ther. 2009;7(7):811-821.
123. Khambadkone S, Coats L, Taylor A, et al. Percutaneous pulmonary valve implantation in humans: results in 59 consecutive patients. Circulation. 2005;112(8):1189-1197.
124. Lurz P, Coats L, Khambadkone S, et al. Percutaneous pulmonary valve implantation: impact of evolving technology and learning curve on clinical outcome. Circulation. 2008;117(15):1964-1972.
125. Andresen B, Døhlen G, Diep LM, Lindberg H, Fosse E, Andersen MH. Psychosocial and clinical outcomes of percutaneous versus surgical pulmonary valve implantation. Open Heart. 2018;5(1):e000758.
126. de Jaegere PP, Kovac J, Otten AM, et al. Abstract 4512: one-year clinical outcome after percutaneous aortic valve implantation. Circulation. 2008;118:S904.
127. Jung HS, Kalva SP, Greenfield AJ, et al. TIPS: comparison of shunt patency and clinical outcomes between bare stents and expanded polytetrafluoroethylene stent-grafts. J Vasc and Interv Radiol. 2009;20(2):180-185.
128. Wang CM, Li X, Fu J, et al. Construction of transjugular intrahepatic portosystemic shunt: bare metal stent/stent-graft combination versus single stent-graft, a prospective randomized controlled study with long-term patency and clinical analysis. Chin Med J (Engl). 2016;129(11):1261-1267.
129. Qi XS, Bai M, Yang ZP, Fan DM. Selection of a TIPS stent for management of portal hypertension in liver cirrhosis: an evidence-based review. World J Gastroenterol. 2014;20(21):6470-6480.
130. Vignalu C, Bargellini, Grosso M, et al. TIPS with expanded polytetrafluoroethylene-covered stent: results of an Italian multicenter study. Am J Roentgenol. 2005;185(2):472-480.
131. Lee JKT, Sagel SS, Stanley RJ, Heiken JP. Computed Body Tomography with MRI Correlation. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2006.
132. Rajagopal M, Venkatesan AM. Image fusion and navigation platforms for percutaneous image-guided interventions. Abdom Radiol (NY). 2016;41(4):620-628.
133. Solbiati M, Passera KM, Rotilio A, et al. Augmented reality for interventional oncology: proof-of-concept study of a novel high-end guidance system platform. Eur Radiol Exp. 2018;2:18.
134. Bhattacharji P, Moore W. Application of real-time 3D navigation system in CT-guided percutaneous interventional procedures: a feasibility study. Radiol Res Pract. 2017;3151694.
135. Solbiati M, Ierace T, Muglia R, et al. Thermal ablation of liver tumors guided by augmented reality: an initial clinical experience. Cancers (Basel). 2022;14(5):1312.
136. Wood BJ, Locklin JK, Viswanathan A, et al. Technologies for guidance of radiofrequency ablation in the multimodality interventional suite of the future. J Vasc Interv Radiol. 2007;18(1 Pt 1):9-24.
137. Mahnken AH, Tacke JA, Wildberger JA, Günther RW. Radiofrequency ablation of osteoid osteoma: initial results with a bipolar ablation device. J Vasc Interv Radiol. 2006;17(9):1465-1470.
138. Brace CL. Microwave Ablation Technology Avoids Problems that Plague RFA, Offers Promise for New Applications. Available at https://www.diagnosticimaging.com/articles/microwave-ablation-technology-avoids-problems-plague-rfa-offers-promise-new-applications. Last accessed May 12, 2022.
139. Simon CJ, Dupuy DE, Mayo-Smith WW. Microwave ablation: principles and applications. Radiographics. 2005;25(Suppl 1):S69-S83.
140. Martin RCG, Scoggins CR, McMasters KM. Safety and efficacy of microwave ablation of hepatic tumors: a prospective review of a 5-year experience. Ann Surg Oncol. 2010;17(1):171-178.
141. Vogl TJ, Roman A, Nour-Eldin NA, Hohenforst-Schmidt W, Bednarova I, Kaltenbach B. A comparison between 915 MHz and 2450 MHz microwave ablation systems for the treatment of small diameter lung metastases. Diagn Interv Radiol. 2018;24(1):31-37.
142. Menon V, Harrington RA, Hichman JS, et al. Thrombolysis and adjunctive therapy in acute myocardial infarction: the seventh ACCP conference on antithrombotic and thrombolytic therapy. Chest. 2004;126(3 Suppl):549S-575S.
143. Wardlaw JM, Zoppo G, Yamaguchi T, Berge E. Thrombolysis for acute ischemic stroke. Cochrane Database Syst Rev. 2003;3:CD000213.
144. Wardlaw JM, Murray V, Berge E, Del Zoppo GJ. Thrombolysis for acute ischaemic stroke. Cochrane Database Syst Rev. 2009;4:CD000213.
145. Adams H, Adams R, Del Zoppo G, Goldstein LB. Guidelines for the early management of patients with ischemic stroke: 2005 guidelines update: a scientific statement from the Stroke Council of the American Heart Association/American Stroke Association. Stroke. 2005;36:916-923.
146. Powers WJ, Rabinstein AA, Ackerson T, et al. 2018 guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2018;49(3):e46-e110.
147. Wardlaw JM, Murray V, Berge E, Del Zoppo GJ. Thrombolysis for acute ischaemic stroke. Cochrane Database Syst Rev. 2014;7:CD000213.
148. Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2019;50(12):e344-e418.
149. American Society for Health-System Pharmacists. AHFS Drug Information, 2019. Bethesda, MD: American Society for Health-System Pharmacists; 2019.
150. Clark WM, Albers GW, Madden KP, Hamilton S. The rtPA (Alteplase) 0- to 6-hour acute stroke trial, part A (A0276g): results of a double-blind, placebo-controlled, multicenter study. Thrombolytic therapy in acute ischemic stroke study investigators. Stroke. 2000;31(4):811-816.
151. Hacke W, Kaste M, Bluhmki E, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med. 2008;359(13):1317-1329.
152. Wahlgren N, Ahmed N, Dávalos A, et al. Thrombolysis with alteplase 3-4.5 h after acute ischaemic stroke (SITS-ISTR): an observational study. Lancet. 2008;372(9646):1303-1309.
153. Ahmed N, Wahlgren N, Grond M, et al. Implementation and outcome of thrombolysis with alteplase 3-4.5 hours after an acute stroke: an updated analysis from SITS-ISTR. Lancet Neurol. 2010;9(9):866-874.
154. U.S. National Library of Medicine. ClinicalTrials.gov. Efficacy and Safety of Desmoteplase to Treat Acute Ischemic Stroke (DIAS-4). Available at https://clinicaltrials.gov/ct2/show/NCT00856661. Last accessed May 12, 2022.
155. Sagonowsky E. Lundbeck Discontinues Further Development of Desmoteplase; 2014 Profit Guidance Range Narrowed. Available at https://www.fiercebiotech.com/biotech/lundbeck-discontinues-further-development-of-desmoteplase-2014-profit-guidance-range. Last accessed May 12, 2022.
156. Reuters. BRIEF: Lundbeck Discontinues Development of Desmoteplase and Narrows 2014 Profit Guidance. Available at https://www.reuters.com/article/hlundbeck-brief-idUSL6N0U209U20141218. Last accessed May 12, 2022.
157. Darcy MD, Cash BD, Feig BW, et al. ACR Appropriateness Criteria: Radiologic Management of Lower Gastrointestinal Tract Bleeding. Reston, VA: American College of Radiology; 2014.
158. Pancioli AM, Broderick J, Brott T, et al. The combined approach to lysis utilizing eptifibatide and rt-PA in acute ischemic stroke: the CLEAR stroke trial. Stroke. 2008;39(12):3268-3276.
159. U.S. Nuclear Regulatory Commission. ALARA. Available at https://www.nrc.gov/reading-rm/basic-ref/glossary/alara.html. Last accessed May 12, 2022.
160. OECD Data. Computed Tomography Exams. Available at https://data.oecd.org/healthcare/computed-tomography-ct-exams.htm. Last accessed May 12, 2022.
161. Smith-Bindman R, Miglioretti DL, Johnson E, et al. Use of diagnostic imaging studies and associated radiation exposure for patients enrolled in large integrated health care systems, 1996–2010. JAMA. 2012;307(22):400-409.
162. Smith-Bindman R, Miglioretti DL, Larson EB. Rising use of diagnostic medical imaging in a large integrated health system. Health Aff. 2008;27(6):1491-1502.
163. Scott BR, Sanders CL, Mitchel REJ, Boreham DR. CT scans may reduce rather than increase the risk of cancer. J Am Physicians Surg. 2008;13(1):8-11.
164. McKinsey and Company. Accounting for the Cost of Health Care in the United States. Available at https://www.mckinsey.com/industries/healthcare-systems-and-services/our-insights/accounting-for-the-cost-of-health-care-in-the-united-states. Last accessed May 12, 2022.
165. Applegate KE, Amis ES Jr, Schauer DA. Radiation exposure from medical imaging procedures. N Engl J Med. 2009;361(23):2289-2292.
166. National Council on Radiation Protection and Measurements. Medical Radiation Exposure of the U.S. Population Greatly Increased Since the Early 1980s. Available at https://www.sciencedaily.com/releases/2009/03/090303125809.htm. Last accessed May 12, 2022.
167. America's Health Insurance Plans. Ensuring Quality through Appropriate Use of Diagnostic Imaging. America's Health Insurance Plans; Washington, DC: 2008.
168. Kouri BE, Parsons RG, Alpert HR. Physician self-referral for diagnostic imaging: review of the empiric literature. Am J Roentgenol. 2002;179(4):843-850.
169. Hendel RC, Cerqueira M, Douglas PS, et al. A multicenter assessment of the use of single-photon emission computed tomography myocardial perfusion imaging with appropriateness criteria. J Am Coll Cardiol. 2010;55(2):156-162.
170. Hughes DR, Bhargavan M, Sunshine JH. Imaging self-referral associated with higher costs and limited impact on duration of illness. Health Aff (Millwood). 2010;29(12):2244-2251.
171. Patel MR, Peterson ED, Dai D, et al. Low diagnostic yield of elective coronary angiography. N Engl J Med. 2010;362(10):886-895.
172. Dick JF 3rd, Gallagher TH, Brenner RJ, et al. Predictors of radiologists' perceived risk of malpractice lawsuits in breast imaging.Am J Roentgenol. 2009;192(2):327-333.
1. KDIGO clinical practice guideline for acute kidney injury. Kidney Int Suppl. 2012;2(1):1-138. Available at https://kdigo.org/guidelines/acute-kidney-injury. Last accessed June 1, 2022.
2. English BS, Ray CE Jr, Chang JY, et al. ACR Appropriateness Criteria: Radiologic Management of Thoracic Nodules and Masses. Reston, VA: American College of Radiology; 2015. Available at https://acsearch.acr.org/docs/69343/Narrative. Last accessed June 1, 2022.
3. Lawton JS, Tamis-Holland JE, Bangalore S, et al. 2021 ACC/AHA/SCAI guideline for coronary artery revascularization: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2022;79(2):e21-e129. Available at https://www.jacc.org/doi/10.1016/j.jacc.2021.09.006. Last accessed June 1, 2022.
4. ASGE Standards of Practice Committee, Chandrasekhara V, Chathadi KV, et al. The role of endoscopy in benign pancreatic disease. Gastrointest Endosc. 2015;82(2):203-214. Available at https://www.giejournal.org/article/S0016-5107(15)02381-0/fulltext. Last accessed June 1, 2022.
5. American College of Radiology. ACR Appropriateness Criteria: Radiologic Management of Lower Gastrointestinal Tract Bleeding. Reston, VA: American College of Radiology; 2020. Available at https://acsearch.acr.org/docs/69457/Narrative. Last accessed June 1, 2022.
Mention of commercial products does not indicate endorsement.