Prior to April 2022, human monkeypox had been a rare zoonotic viral exanthem occasionally encountered in persons living in West or Central Africa, or in persons having had contact with imported animals or recent travel to countries where the disease occurs. Within the span of six weeks, from mid-April to June 1, 2022, single case and clusters of confirmed human monkeypox were reported in 28 countries on multiple continents, including the United States (nine states), none of which are endemic for the disease. On July 23, 2022, the World Health Organization (WHO) declared that the current global monkeypox outbreak constitutes a Public Health Emergency of International Concern (PHEIC). Given the rarity of cases previously encountered in the United States, clinical care providers and public health professionals may be unfamiliar or unaware of the clinical features and natural history of monkeypox, including risk factors, modes of transmission, diagnosis, and management of cases occurring in relation to the current outbreak. This course addresses these potential gaps in knowledge in order to improve patient care and outcomes.
This course is designed for physicians, physician assistants, nurses, pharmacy professionals, and other healthcare professionals who may identify and care for patients with suspected or confirmed human monkeypox infection.
The purpose of this course is to address these knowledge gaps to enable timely diagnosis, treatment, and prevention of monkeypox, thereby promoting public health strategies to limit spread of the outbreak.
Upon completion of this course, you should be able to:
- Outline the epidemiology and background of monkeypox virus globally and in the United States.
- Describe the transmission, course, and clinical presentation of monkeypox virus disease.
- Discuss the diagnosis and treatment of monkeypox infections.
- Analyze measures that may effectively prevent transmission of monkeypox virus.
John M. Leonard, MD, Professor of Medicine Emeritus, Vanderbilt University School of Medicine, completed his post-graduate clinical training at the Yale and Vanderbilt University Medical Centers before joining the Vanderbilt faculty in 1974. He is a clinician-educator and for many years served as director of residency training and student educational programs for the Vanderbilt University Department of Medicine. Over a career span of 40 years, Dr. Leonard conducted an active practice of general internal medicine and an inpatient consulting practice of infectious diseases.
Contributing faculty, John M. Leonard, MD, has disclosed no relevant financial relationship with any product manufacturer or service provider mentioned.
John V. Jurica, MD, MPH
Jane C. Norman, RN, MSN, CNE, PhD
Randall L. Allen, PharmD
The division planners have disclosed no relevant financial relationship with any product manufacturer or service provider mentioned.
Sarah Campbell
The Director of Development and Academic Affairs has disclosed no relevant financial relationship with any product manufacturer or service provider mentioned.
The purpose of NetCE is to provide challenging curricula to assist healthcare professionals to raise their levels of expertise while fulfilling their continuing education requirements, thereby improving the quality of healthcare.
Our contributing faculty members have taken care to ensure that the information and recommendations are accurate and compatible with the standards generally accepted at the time of publication. The publisher disclaims any liability, loss or damage incurred as a consequence, directly or indirectly, of the use and application of any of the contents. Participants are cautioned about the potential risk of using limited knowledge when integrating new techniques into practice.
It is the policy of NetCE not to accept commercial support. Furthermore, commercial interests are prohibited from distributing or providing access to this activity to learners.
Supported browsers for Windows include Microsoft Internet Explorer 9.0 and up, Mozilla Firefox 3.0 and up, Opera 9.0 and up, and Google Chrome. Supported browsers for Macintosh include Safari, Mozilla Firefox 3.0 and up, Opera 9.0 and up, and Google Chrome. Other operating systems and browsers that include complete implementations of ECMAScript edition 3 and CSS 2.0 may work, but are not supported. Supported browsers must utilize the TLS encryption protocol v1.1 or v1.2 in order to connect to pages that require a secured HTTPS connection. TLS v1.0 is not supported.
The role of implicit biases on healthcare outcomes has become a concern, as there is some evidence that implicit biases contribute to health disparities, professionals' attitudes toward and interactions with patients, quality of care, diagnoses, and treatment decisions. This may produce differences in help-seeking, diagnoses, and ultimately treatments and interventions. Implicit biases may also unwittingly produce professional behaviors, attitudes, and interactions that reduce patients' trust and comfort with their provider, leading to earlier termination of visits and/or reduced adherence and follow-up. Disadvantaged groups are marginalized in the healthcare system and vulnerable on multiple levels; health professionals' implicit biases can further exacerbate these existing disadvantages.
Interventions or strategies designed to reduce implicit bias may be categorized as change-based or control-based. Change-based interventions focus on reducing or changing cognitive associations underlying implicit biases. These interventions might include challenging stereotypes. Conversely, control-based interventions involve reducing the effects of the implicit bias on the individual's behaviors. These strategies include increasing awareness of biased thoughts and responses. The two types of interventions are not mutually exclusive and may be used synergistically.
#94040: Monkeypox: The 2022 Global Outbreak
Before April 2022, human monkeypox was a rare viral zoonotic disease endemic to West and Central Africa [1,2]. The disease, first recognized in 1970, resembled smallpox clinically but differed epidemiologically. It was recognized that smallpox vaccination protected against monkeypox virus infection, as the majority of reported cases were unvaccinated children younger than 10 years of age. Secondary spread among susceptible close contacts was distinctly uncommon (5%), much lower than that reported from smallpox (25% to 40%) [3]. Human monkeypox occurred infrequently, and the spread of disease among susceptible close contacts was limited, suggesting the virus was not sufficiently transmissible to permit sustained propagation of infection in humans. Thus, monkeypox disease was not considered to be an important public health problem [3].
In the short period from mid-April to June 1, 2022, single cases and clusters of confirmed monkeypox were reported to the World Health Organization (WHO) from 28 countries across multiple regions, including the United States, none of which are endemic for the disease. Demographic data showed significant deviation from the usual epidemiologic characteristics of endemic monkeypox. On July 23, 2022, in response to an alarming increase in reported cases and locales affected, the WHO declared that the current global monkeypox outbreak constitutes a Public Health Emergency of International Concern (PHEIC) [1].
Given the rarity of cases previously encountered in the United States, clinical care providers and public health professionals may be unfamiliar or unaware of the clinical features and natural history of monkeypox, including risk factors, modes of transmission, and diagnosis and management of cases occurring in relation to the current outbreak. The objective of this course is to address these knowledge gaps to enable timely diagnosis, treatment, and prevention of monkeypox, thereby promoting public health strategies to limit spread of the outbreak.
Monkeypox virus is so-named for its discovery in 1958 as the cause of a pox-like disease outbreak among captive monkeys housed at the State Serum Institute in Copenhagen, Denmark [2]. The actual source of the monkeypox virus is unknown, though African rodents, including squirrels, are considered likely reservoirs in nature. During the period 1970–1979, 47 human cases of a smallpox-like disease were detected in smallpox-free areas near tropical rain forests in West and Central Africa [3]. Virologic studies revealed that the disease was caused by monkeypox virus, an animal orthopoxvirus known to circulate among small animals and non-human primates. In subsequent years, sporadic cases of human monkeypox were attributed to zoonotic (animal-to-human) transmission; cases reported in persons living outside Africa were linked to contact with imported animals or recent travel to countries where the disease occurs [1]. From 2018 to 2022, isolated cases of monkeypox were reported among travelers from Nigeria to Israel, the United Kingdom, Singapore, and the United States [1].
Monkeypox virus is a member of the orthopoxvirus family of viruses, the same family as variola virus, the cause of smallpox. Symptoms and signs are similar to smallpox but milder, and case fatalities are rare. The characteristic clinical syndrome begins with systemic symptoms, fever, and lymphadenopathy followed by the onset of a striking papulovesicular skin eruption of varying severity. Absent complications (e.g., pneumonitis, encephalitis, secondary bacterial skin and soft tissue infection), the illness tends to resolve in two to four weeks. In the decades before smallpox eradication in 1980, prevailing natural and vaccine immunity to variola within population groups provided immune cross-protection against related orthopoxvirus infections, including monkeypox [2,3]. During this period of widespread attention to variola, clinical recognition of other pox-like infections was obscured, and occasional intercurrent cases of monkeypox were likely attributed to mild smallpox [1].
In past decades, human-to-human transmission of monkeypox virus was known to occur among household contacts and prison populations. However, chains of transmission were short and unsustainable [2,3]. An analysis of data on human monkeypox in the Democratic Republic of Congo (DRC, formerly Zaire) for the period 1981 to 1986 found that among 2,278 persons who had close contact with 245 patients with monkeypox infected from an animal source, 93 subsequently became ill and were presumed to have acquired infection from a known human source [4]. Of the 93 secondary infections, 69 were spread in the first generation, 19 in the second generation, and the remaining 5 cases in the third and fourth generations. The overall probability of acquiring monkeypox from exposure to a known human source was 3%. Household spread was the predominant locus of secondary transmission, and the highest attack rate (11.7%) occurred in children younger than 5 years of age. These findings indicated that human spread of monkeypox was limited and appeared to require prolonged or repeated exposure to open skin lesions or virus-laden debris in the environment.
The first reported monkeypox outbreak outside Africa occurred in the United States in 2003. An investigation identified 47 confirmed cases, including many children, linked to contact with infected pet prairie dogs recently housed with small animals imported from Ghana [1]. This outbreak demonstrated that monkeypox virus circulating in intermediate hosts could be transferred from one animal to another and subsequently to humans. There were two cases of possible human spread, though the possibility of transmission from an infected pet could not be excluded. In 2018, a case of secondary infection was reported in a healthcare worker exposed to an imported case of monkeypox in the United Kingdom. Transmission was attributed to physical contact with contaminated bedding, and infection control and contact precautions were implemented. An investigation of 134 potential contacts identified 4 additional secondary cases of monkeypox, all of whom survived [5].
Since eradication of smallpox and termination of routine vaccination in 1980, the epidemiology of orthopoxviruses has changed and monkeypox has emerged as a public health issue of broader concern [6]. Population groups appear to have become more vulnerable to monkeypox, as evidenced by a progressive increase in the number of reported cases and small outbreaks in endemic areas. Following the identification of human monkeypox in 1970, 48 confirmed cases in six African countries were reported during the next decade (1970–1979), increasing to 343 in the 1980s, and 520 in the 1990s [7]. Factors hypothesized for the emergence of human monkeypox include rain forest exploitation, climate change, armed conflicts in disease areas, and waning herd immunity following cessation of smallpox vaccination [6]. Using ecological niche modeling techniques in conjunction with climate and remote sensing variables, investigators have tried to predict animal reservoir species distribution and the spread of human monkeypox virus in Africa's Congo Basin. Results show that forest clearing and climate change are major factors driving the transmission of virus from wildlife to humans under current climate conditions [8].
While deforestation and urbanization have increased incidental human contact with infected rodents, populations have also become more susceptible to monkeypox because of waning herd immunity following cessation of smallpox vaccination in 1980. Previously, vaccination against smallpox with first-generation vaccinia-based vaccine was shown to be 85% effective in preventing monkeypox [1]. An analysis of data collected on 91 human monkeypox cases during the 1980s found that the secondary attack rate for contacts without a vaccination scar (4.3%) differed significantly from those who had been vaccinated in the past (0.7%) [3].
As of September 7, 2022, 54,707 confirmed cases of monkeypox, including 18 deaths, have been reported to WHO this year from 102 Member States across all WHO regions [9]. This is the first time that cases and sustained chains of transmission have been reported in countries without direct epidemiologic links to areas of West or Central Africa. The most affected countries globally are the United States (n=19,833), Spain (n=6,749), Brazil (n=5,523), France (n=3,646), Germany (n=3,505), and the United Kingdom (n=3,484).
Data reported to the WHO reveal several key epidemiological findings [9]. The outbreak affects young people of male gender; of those cases with available data on gender, 98% are males, with a median age of 36 years. Among cases with sexual orientation reported, 96% identified as men who have sex with men. Of all reported modes of transmission, a sexual encounter was reported most commonly (85%) as the suspected transmission event. The majority of persons infected were likely exposed in a party setting with sexual contacts, which accounted for 61% of all likely exposure categories reported. Among cases with known human immunodeficiency virus (HIV) status, 45% are HIV positive. Of all cases reported to WHO with available data, 1.9% are female; of these, the most commonly reported exposure setting was the household (32%) and most common form of transmission was via sexual encounters [9].
The Centers for Disease Control and Prevention (CDC) has been closely tracking cases of monkeypox detected in the United States since mid-May 2022. As of September 12, 2022, 21,985 confirmed monkeypox/orthopoxvirus cases have been reported [10]. The cumulative number of cases by state varies directly with the population density; more than 1,000 cases have been reported from New York, Illinois, Florida, Georgia, Texas, and California.
Several factors of public health importance are thought to be driving the current global monkeypox outbreak: biologic changes in the virus that affect transmission; waning of herd immunity to smallpox; changes in human behavior, such as relaxation of COVID-19 preventive measures and resumption of international travel; and sexual interactions associated with large gatherings, suggesting an amplification of transmission through sexual networks [11]. Women and children account for a small (~2%) subset of cases, indicating the potential for wider spread and the propensity for anyone to become infected who has been in close contact with someone who has monkeypox.
Orthopoxviruses are large, double-stranded DNA viruses within the genus Orthopoxvirus, family Poxviridae. Orthopoxvirus species include Variola virus, Vaccinia virus, Monkeypox virus, and Cowpox virus. Infection with one orthopoxvirus or immunization with an orthopoxvirus vaccine induces immunologic cross-protection against other species of virus in the genus [6]. A variety of animals have been identified as susceptible to monkeypox virus infection, including squirrels, Gambian pouched rats, dormice, non-human primates, and other species [1]. The source reservoir, pattern of monkeypox virus circulation in nature, and human behaviors that facilitate zoonotic transmission have not been clearly determined.
Genomic sequencing has verified the existence of two geographically distinct clades of monkeypox virus: the central African (Congo Basin) clade, which is more severe and has a case fatality rate near 10%; the West African clade, which is less severe and has a mortality of 1% [1]. All human monkeypox outside Africa, including the current global outbreak has been caused by descendants of the West African clade. In November 2022, the WHO announced that it would be referring to monkeypox as mpox; both names will be used simultaneously for one year while "monkeypox" is phased out [24]. They have also updated the citations used in reference to each clade variant. The Congo Basin clade is now referred to as Clade I; the West African derivative is now Clade II, with subclades IIa and IIb [1].
Animal-to-human (zoonotic) transmission can occur from direct contact with the blood, bodily fluids, or cutaneous or mucosal lesions of infected animals [1]. Eating inadequately cooked meat and other animal products of infected animals is a possible risk factor [1].
Unlike endemic case clusters of monkeypox previously reported, human-to-human transmission is common in the 2022 outbreak and accounts for the scope and rapidity of spread. As indicated, human spread of monkeypox occurs through close, sustained physical contact that permits direct exposure to body fluids or material from open skin and mucosal lesions. Examples of intermediate- and high-risk exposures associated with the 2022 monkeypox outbreak include [10]:
Direct contact with infectious skin lesions or scabs (including during sexual contact, kissing, cuddling, or holding hands)
Exposure to large respiratory droplets during prolonged face-to-face or mouth-to-mouth contact, or by close proximity to coughing or sneezing of an individual with active infection
Contact with contaminated clothing, bed linens, or towels used by an infected person (fomite transmission)
If contaminated clothing or linens are shaken, infectious particles may be dispersed into the air and inhaled or land on mucosal membranes. The precaution of wearing an N95 mask or equivalent respirator is recommended during any procedure that may create aerosols from oral secretions, skin lesions, or suspensions of dried exudates [10]. Patients with monkeypox are considered infectious from the time of symptom onset until the skin lesions have crusted.
There is potential risk for vertical (transplacental) transmission of monkeypox to the unborn fetus, evidenced by a report of two miscarriages and one case of fatal congenital monkeypox disease following infection during pregnancy [12].
Published clinical case studies have further characterized the role of intimate physical contact via sexual activity in the spread of monkeypox associated with the 2022 outbreak. In a clinical case series of 528 infections diagnosed between April 27 and June 24, 2022, at 43 sites across 16 countries, 98% of the patients were gay or bisexual men [11]. The suspected mode of monkeypox transmission reported by the examining clinician was sexual close contact in 95% of the persons with infection. The likelihood of sexual transmission was supported by the presence of primary genital, anal, and oral mucosal lesions, considered to represent the inoculation site. Although monkeypox virus DNA was detectable by polymerase chain reaction (PCR) in seminal fluid from 29 of 32 cases in which samples were submitted, it is not yet known whether the presence of viral DNA in semen reflects replication-competent monkeypox virus capable of transmitting the infection. Among 406 patients with a recorded sexual history, 147 (28%) reported travel abroad in the month before diagnosis, and 103 (20%) had attended large gatherings (more than 30 persons), such as Pride events [11].
The incubation period of monkeypox is 5 to 21 days [1]. As noted, illness usually begins with a prodromal phase of fever, malaise, headache, myalgias, and lymphadenopathy. This is followed in one to five days by the onset of a maculopapular skin eruption and/or mucosal lesions, most pronounced on the face and extremities. According to WHO 2022 outbreak data, the most common sites for skin and mucosal lesions are face (95%), palms and soles (75%), oral mucus membranes (70%), genitalia (30%), and conjunctivae (20%) [1]. Typically, the skin lesions progress in stages from maculopapular to papulovesicular to umbilicated pustules before crusting over and desquamating within a period of two to four weeks. Unusual features of the rash associated with the current outbreak include the following: mucosal lesions more numerous than previously described; lesions confined to atypical locations, such as the genital or perineal/perianal area, as well as the mouth and eyes; and development of rash or mucosal lesions prior to onset of constitutional symptoms [1].
In the 2022 clinical review of 528 monkeypox cases across multiple countries, common systemic symptoms preceding the rash included fever (62%), lethargy (41%), myalgia (31%), and headache (27%); lymphadenopathy was reported in 56% [11]. Seventy (13%) patients were admitted to a hospital for infection control purposes or management of complications. The most common medical reasons for admission were management of pain (21 persons), mostly for severe anorectal pain, and treatment of soft-tissue superinfection [18]. Other reasons included severe pharyngitis limiting oral intake (5 persons), eye lesions (2 persons), acute kidney injury (2 persons), and myocarditis (2 persons).
The possibility of monkeypox should be considered in any patient with compatible clinical syndrome (e.g., any combination of fever, rash, lymphadenopathy) and epidemiologic risk factors, such as travel or animal exposure connected to endemic areas of virus circulation or recent history of sexual activity involving persons known or suspected of monkeypox disease. The differential diagnosis includes other infections that present with generalized or focal skin lesions (e.g., herpes, varicella zoster, secondary syphilis, acute streptococcal or meningococcal infection). The presence of lymphadenopathy helps distinguish monkeypox from other, similar viral exanthems (e.g., varicella zoster, chickenpox). The laboratory diagnosis of monkeypox relies on DNA PCR testing of specimens (scrapings) obtained from skin or mucosal lesions. PCR testing of blood samples are usually inconclusive because of the short duration of viremia relative to the timing of specimen collection [1]. Serologic testing is unreliable for monkeypox-specific confirmation because of common cross-reactivity with other orthopoxviruses and vaccination.
The CDC recommends careful attention to the following epidemiologic criteria, within 21 days of illness onset, when assessing a patient with suspected monkeypox [13]:
Reports having contact with a person or people with a similar appearing rash or who received a diagnosis of confirmed or probable monkeypox
Had close or in-person contact with individuals in a social network experiencing monkeypox activity; this includes men who have sex with men and meet partners through an online website, digital application ("app"), or social event/gathering
Traveled outside the United States to a region with known confirmed cases or country where monkeypox is endemic
Had contact with a dead or wild animal or exotic pet known to be an African endemic species or used a product derived from such animals (e.g., game meat, creams, lotions, powders)
For purposes of reporting and public health response to the 2022 outbreak, the CDC defines monkeypox cases as suspect, probable, or confirmed [13]. A suspect case is one with new-onset characteristic rash or meets one of the epidemiologic criteria and has a high clinical suspicion for monkeypox. A probable case is one having no suspicion of other recent orthopoxvirus exposure in which there is laboratory evidence of active orthopoxvirus infection demonstrated by PCR, immunochemical, or electron microscopy, or the presence of detectable anti-orthopoxvirus immunoglobulin M (IgM) antibody within 4 to 54 days after onset of rash. A confirmed case of monkeypox requires demonstration of the presence of monkeypox virus DNA by PCR testing or next-generation sequencing of a clinical specimen or isolation of the virus in culture from a clinical specimen [13].
The characteristic skin eruption of monkeypox disease exhibits the following features: deep-seated and well-circumscribed lesions, often with central umbilication (Image 1), and lesion progression through specific sequential stages—macules, papules, vesicles, pustules, and scabs. It is sometimes confused with other diseases that are more commonly encountered in clinical practice (e.g., secondary syphilis, herpes, varicella zoster). Historically, sporadic accounts of patients co-infected with monkeypox virus and other infectious agents (e.g., varicella zoster, syphilis) have been reported, so patients with skin lesions typical for monkeypox should be considered for testing, even if other tests are already positive [13]. Key characteristics for identifying monkeypox rash, including instructive photographic images of skin lesions in sequential stages, are provided at the CDC website, accessible at https://www.cdc.gov/poxvirus/monkeypox/clinicians/clinical-recognition.html [14].

Procedures for safe collection and transport of specimens, including specimen collection printouts for testing patients for monkeypox, are available through the CDC [15]. Effective communication and precautionary measures between collection teams and laboratory staff are emphasized. Personnel who collect specimens should use personal protective equipment (PPE) in accordance with recommendations for healthcare settings.
For initial laboratory testing of monkeypox virus specimens at Laboratory Response Network (LRN) laboratories or authorized commercial laboratories, the recommended specimen type is lesion material (i.e., swab of lesion surface or crust from healing lesion). Specifics on the acceptable specimen type within these laboratories may vary. Providers should contact the appropriate public health department or commercial laboratory to determine acceptable specimens. The CDC has prepared two 1-page illustrated printouts (in PDF form for posting in office or clinic) with instructions for monkeypox diagnostic testing and techniques for specimen collection. These printouts are accessible at https://www.cdc.gov/poxvirus/monkeypox/clinicians/prep-collection-specimens.html.
In general, specimens should be collected in the following manner, using a plastic, sterile, leak-proof container for specimen collection [15]. Select two or three lesions from different locations on the body or from lesions that differ in appearance. Two swabs from each lesion should be collected for testing. Using two sterile synthetic swabs with a plastic, wood, or thin aluminum shaft, swab the lesion vigorously at least two to three times on each side of the swab to collect adequate material for DNA testing. Do not use cotton swabs. The CDC suggests it is not necessary to de-roof the lesion before swabbing, but if the lesion ruptures while swabbing, ensure that swab collects lesion fluid. Break off the end of each swab's applicator into a 1.5- or 2-mL screw-capped tube with O-ring or place the entire swab into a sterile container that has a gasket seal in order to be shipped under required conditions [15].
Specimen collection, storage, and shipping of human specimens is subject to certain restrictions and requires a designated request form with each specimen. Clinician providers should consult with appropriate laboratory personnel to assure proper procedure [15].
Many patients with monkeypox follow a mild, self-limited course, requiring only symptomatic treatment combined with measures aimed at limiting spread of infection. The prognosis for monkeypox depends on multiple factors, such as previous vaccination status, general health status, presence of comorbidities and concurrent medications. At present, no antiviral therapeutic agent has been approved specifically for treatment of monkeypox virus infection. However, antiviral drugs developed for use in patients with smallpox may be beneficial against monkeypox [16].
Patients who should be considered for treatment following consultation with the CDC might include those with severe disease and/or complications requiring hospitalization; persons at high risk of severe disease because of immunocompromise (e.g., HIV, hematologic malignancy, immunosuppressive therapies); patients with aberrant infections involving anatomic areas that pose a specific hazard, such as the eyes (e.g., keratoconjunctivitis), genitals, and anus [16]. Other population groups possibly at risk for severe disease include pediatric patients, especially those younger than 8 years of age, pregnant or breastfeeding women, and persons with the history or presence of serious skin disorders (e.g., atopic dermatitis, eczema, herpes zoster). Healthcare providers should consult CDC Interim Clinical Guidance for the Treatment of Monkeypox, which includes the use of medical countermeasures available through the Strategic National Stockpile (SNS) [16]. Treatment options available through the SNS include two antiviral agents (tecovirimat and cidofovir) and vaccinia immune globulin intravenous (VIGIV).
Tecovirimat (TPOXX) is an antiviral medication approved by the U.S. Food and Drug Administration (FDA) for the treatment of smallpox in adults and children. Data are not available on the effectiveness of tecovirimat in treating monkeypox in humans, but animal studies have shown it to be effective in treating infections caused by orthopoxviruses [17]. Human clinical trials have found the drug to be safe with only minor side effects. Small case studies of individuals infected with monkeypox virus suggest that tecovirimat may shorten the duration of illness and viral shedding [17,18]. The CDC holds an expanded access protocol (sometimes called compassionate use) that allows for dispensing stockpiled tecovirimat to treat monkeypox during an outbreak. Tecovirimat is formulated as an oral capsule (200 mg) and as a solution for intravenous administration.
The CDC, in partnership with the FDA, has streamlined the process of obtaining tecovirimat, allowing healthcare providers to start treatment before paperwork is completed. Multiple state health and territorial departments are pre-positioning supplies of tecovirimat within their jurisdictions. Clinicians and care facility pharmacists requesting tecovirimat should contact their state/territorial health department. For questions regarding urgent situations after hours and on weekends, providers may contact the CDC through the CDC Emergency Operations Center (770-488-7100) to talk with a clinician. Additional information on the process for requesting tecovirimat and the CDC guidance regarding patient selection, efficacy, formulations, adverse reactions and drug-drug interactions may be accessed at https://www.cdc.gov/poxvirus/monkeypox/clinicians/obtaining-tecovirimat.html [18].
VIGIV is licensed by the FDA for the treatment of complications due to vaccinia vaccination including eczema vaccinatum and generalized vaccinia, among other complications. The CDC holds an expanded access protocol that allows the use of VIGIV for the treatment of orthopoxviruses (including monkeypox) in an outbreak. Data are not available on the effectiveness of VIG in the treatment of monkeypox, and it is unknown whether a patient with severe disease will benefit from treatment [12]. However, healthcare providers may consider its use in severe cases.
VIG can be considered for prophylaxis against monkeypox in an exposed person with severe immunodeficiency in T-cell function for which smallpox vaccination following exposure to monkeypox virus is contraindicated [12].
When properly administered before an exposure, vaccines previously developed and stockpiled for prevention of smallpox are effective at protecting people against monkeypox virus infection. Vaccines may also be effective for post-exposure prophylaxis if given within four days from the date of exposure [1,19]. If given between 4 to 14 days after exposure, vaccination may reduce symptoms and severity of disease. ACAM2000 and JYNNEOS (also known as Imvamune or Imvanex) are the two licensed smallpox vaccines in the United States. The CDC has prepared vaccine guidance for healthcare professionals on prevention of monkeypox, including interim clinical considerations for using JNNEOS and ACAM2000 vaccines during the 2022 monkeypox outbreak [19,20].
ACAM2000 is an attenuated, self-replicating live vaccine. It carries some risk of dissemination and is not safe for use in persons with immunodeficiency syndromes. JYNNEOS is a third-generation vaccine based on an attenuated, non-replicating live orthopoxvirus, Modified Vaccinia Ankara (MVA) [20]. MVA does not replicate efficiently in humans and has a better safety profile. The JYNNEOS vaccine is the primary vaccine being used during the 2022 monkeypox outbreak in the United States. Although JYNNEOS is routinely administered subcutaneously, a smaller dose administered by intradermal injection is considered equally effective and conserves the limited available supplies of this vaccine. No clinical trial data are available on the effectiveness of either vaccine in the current global outbreak; the effectiveness of JYNNEOS in preventing or ameliorating monkeypox disease has been concluded from a clinical study on the immunogenicity of JYNNEOS and efficacy data from animal studies [19]. People who are vaccinated should continue to take steps to protect themselves from infection by avoiding close, skin-to-skin contact, including intimate contact, with someone who has monkeypox.
ACAM2000 is licensed as a single dose. It is administered as a live vaccinia virus preparation that is inoculated into the skin by pricking the skin surface [19]. Following a successful inoculation, a lesion will develop at the site of the vaccination (i.e., a "take"). Replicating virus from the inoculation site may spread to other parts of the body or even to other people; therefore, individuals who receive vaccination with ACAM2000 must take precautions to prevent spread [19]. Adverse events following ACAM2000, including myopericarditis or vaccinia virus transmission to household contacts, can be serious [20]. ACAM2000 will be made available for individuals who decide in consultation with their healthcare provider that the potential benefits of vaccination outweigh potential risks from adverse events [20].
The JYNNEOS vaccine is licensed as a series of two doses administered 28 days (4 weeks) apart for use in adults 18 years of age and older. There is no visible "take" and no risk of spread to other parts of the body or other people [19]. The standard regimen involves a subcutaneous injection volume of 0.5 mL [20]. People who receive JYNNEOS are not considered vaccinated until two weeks after they receive the second dose of the vaccine.
In the context of the current national Public Health Emergency (PHE), an alternative regimen to subcutaneous JYNNEOS vaccine administration may be used. The authorized alternative regimen involves an intradermal route of administration with an injection volume of 0.1 mL. This approach could increase the number of available JYNNEOS vaccine doses by up to five-fold. Results from a clinical study showed that the lower intradermal dose was immunologically non-inferior to the standard subcutaneous dose [20].
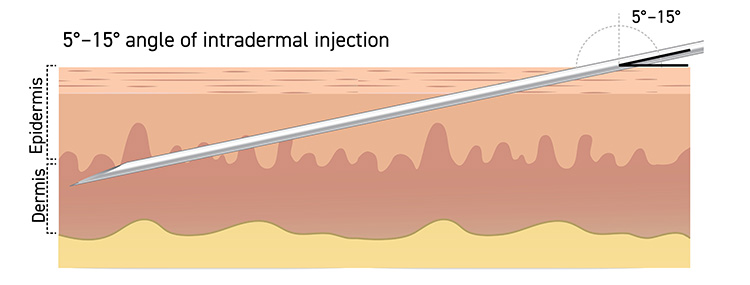
Intradermal administration involves injecting the vaccine superficially between the epidermis and the hypodermis layers of the skin, typically of the volar aspect (inner side) of the forearm. After an appropriate location is located, it should be cleaned. The skin is pulled taut, and the needle is positioned with the bevel up. The needle should be inserted at a 5- to 15-degree angle into the dermis (Figure 1). The solution should then be slowly injected into the dermis. This should produce a noticeable pale elevation of the skin (wheal). All patients should be observed for at least 15 minutes following vaccination; patients with a history of anaphylaxis to chicken, egg protein, gentamicin, or ciprofloxacin should be observed for 30 minutes. The technique requires prior experience or training in order to ensure it is done properly; otherwise, such a small volume of vaccine delivered into the subcutaneous layer may not elicit an optimal immune response.
The following video, produced by the CDC, demonstrates the correct technique for administering JYNNEOS intradermally.
Additional teaching tools, including stepwise color images, are provided at the CDC website, accessible at https://www.cdc.gov/poxvirus/monkeypox/interim-considerations/jynneos-vaccine.html.
Recipients should be informed of the risks and benefits of JYNNEOS prior to vaccination. Healthcare providers should review CDC guidance on pre- and post-vaccination counseling, including side effects and safety considerations [20]. Local side effects (e.g., pain, erythema, edema) are more severe with intradermal than subcutaneous administration. It is important to determine the medical and allergy history of recipients to appropriately decide whether to administer the vaccine subcutaneously or intradermally. JYNNEOS vaccine contains small amounts of gentamicin and ciprofloxacin and is produced using chicken embryo fibroblast cells [20]. Recipients should be counseled about possible side effects from vaccination and be provided with a JYNNEOS vaccine information statement or FDA JYNNEOS EUA Fact Sheet, as applicable.
In order to control the current global monkeypox outbreak, it is necessary to stop human-to-human transmission. To that end, the WHO has issued interim guidance for disease surveillance, case investigation, and contact tracing for monkeypox [21]. The objectives of surveillance and case investigation are to rapidly identify cases and clusters in order to provide optimal care; to isolate cases to prevent further transmission; to identify, manage, and follow-up contacts in order to recognize early signs of infection; to protect frontline health workers; and to tailor effective control and prevention measures [21].
Clinicians should report suspected, probable, and confirmed monkeypox cases immediately to local or state public health authorities. A minimum dataset of epidemiologically relevant information should be included so contact and contact tracing can be initiated as soon as possible. Contacts of cases should be monitored (or self-monitor) daily for signs or symptoms for a period of 21 days [21].
The CDC recommends that patients with monkeypox remain isolated at home or at another location for the duration of illness, but this may not be possible in all situations [22]. Current data suggest people can spread monkeypox from the time symptoms start until all symptoms have resolved, including full healing of the rash with formation of a fresh layer of skin. Ideally, people with monkeypox would remain in isolation for the duration of illness, which typically lasts two to four weeks. However, if a person with monkeypox is unable to remain fully isolated throughout the illness, they should do the following [22]:
Remain isolated at home while symptomatic.
Avoid close or physical contact with others, including sexual and/or close intimate contact.
Cover lesions.
Wear a well-fitting mask when interacting with others.
Avoid public transportation when leaving home.
While rash persists, cover all parts with clothing, gloves, or bandages.
Until all signs and symptoms have resolved, do not share items that have been worn or handled with other people or animals and avoid sharing utensils, cups, and other personal use items.
General guidance for prevention of monkeypox, including personal protection, safe sex and social gatherings, pets and monkeypox, and congregate settings is available from the CDC [23]. As of September 2022, data suggest that gay, bisexual, and other men who have sex with men make up the majority of cases in the current monkeypox outbreak. However, anyone, regardless of sexual orientation or gender, who has been in close personal contact with someone who has monkeypox is at risk [23].
It is important for healthcare professionals to give patients explicit verbal and written instructions on management of monkeypox symptoms and prevention of transmission. Patients' health literacy is typically low, and patients whose primary language is not English, racial/ethnic minorities, and patients older than 60 years of age have the lowest health literacy. Many patients report that the clinician did not provide information in words they could understand, and some individuals feel shame about their lack of understanding and fail to ask for clarification due to embarrassment. Non-English-proficient patients require a professional translator (i.e., not a family member) to be present at each visit. It is vital that the patient understand the importance of precisely following transmission prevention measures.
| Centers for Disease Control and Prevention |
| https://www.cdc.gov/poxvirus/monkeypox |
| National Institute of Allergy and Infectious Diseases |
| https://www.niaid.nih.gov/diseases-conditions/monkeypox |
| U.S. Food and Drug Administration |
| https://www.fda.gov/emergency-preparedness-and-response/mcm-issues/fda-monkeypox-response |
| World Health Organization |
| https://www.who.int/emergencies/situations/monkeypox-oubreak-2022 |
1. World Health Organization. Monkeypox. Available at https://www.who.int/news-room/fact-sheets/detail/monkeypox. Last accessed September 14, 2022.
2. Di Giulio DB, Eckburg PB. Human monkeypox: an emerging zoonosis. Lancet Infect Dis. 2004;4:15-25.
3. Jezek Z, Gromyko AI, Szczeniowski MV. Human monkeypox. J Hyg Epidemiol Microbiol Immunol. 1983;27:13-28.
4. Jezek Z, Grab B, Szczeniowski MV, et al. Human monkeypox: secondary attack rates. Bull World Health Organ. 1988;66:465-470.
5. Vaughan A, Aarons E, Astbury J, et al. Human-to-human transmission of monkeypox virus, United Kingdom, October 2018.Emerg Infect Dis. 2020;26:782-785.
6. Simpson K, Heymann D, Brown CS, et al. Human monkeypox—after 40 years, an unintended consequence of smallpox eradication. Vaccine. 2020;38:5077-5081.
7. Stacey J. Monkeypox virus outbreak: can evolution guide us to new treatments or vaccines? eBioMedicine 2022;82:104221.
8. Thomassen HA, Fuller T, Asefi-Najafabady S, et al. Pathogen-host associations and predicted range shifts of human monkeypox in response to climate change in central Africa. PLoS One. 2013;8(7):e66071.
9. World Health Organization. 2022 Monkeypox Outbreak: Global Trends. Available at https://worldhealthorg.shinyapps.io/mpx_global. Last accessed September 14, 2022.
10. Centers for Disease Control and Prevention. Monkeypox: 2022 Outbreak. Available at https://www.cdc.gov/poxvirus/monkeypox. Last accessed September 14, 2022.
11. Thornhill JP, Barkati S, Walmsley S, et al. Monkeypox virus infection in humans across 16 countries—April–June 2022. N Engl J Med. 2022;387:679-691.
12. Mbala PK, Huggins JW, Riu-Rovira T, et al. Maternal and fetal outcomes among pregnant women with human monkeypox infection in the Democratic Republic of Congo. J Infect Dis 2017;216:824-828.
13. Centers for Disease Control and Prevention. Case Definitions for Use in the 2022 Monkeypox Response. Available at https://www.cdc.gov/poxvirus/monkeypox/clinicians/case-definition.html. Last accessed September 14, 2022.
14. Centers for Disease Control and Prevention. Monkeypox: Clinical Recognition. Available at https://www.cdc.gov/poxvirus/monkeypox/clinicians/clinical-recognition.html. Last accessed September 14, 2022.
15. Centers for Disease Control and Prevention. Monkeypox: Preparation and Collection of Specimens. Available at https://www.cdc.gov/poxvirus/monkeypox/clinicians/prep-collection-specimens.html. Last accessed September 14, 2022.
16. Centers for Disease Control and Prevention. Monkeypox: Treatment Information for Healthcare Professionals. Available at https://www.cdc.gov/poxvirus/monkeypox/clinicians/treatment.html. Last accessed September 14, 2022.
17. Centers for Disease Control and Prevention. Guidance for Tecovirimat Use Under Expanded Access Investigational New Drug Protocol during 2022 U.S. Monkeypox Cases. Available at https://www.cdc.gov/poxvirus/monkeypox/clinicians/Tecovirimat.html. Last accessed September 14, 2022.
18. Centers for Disease Control and Prevention. Clinical Guidance, Information for Healthcare Providers on Obtaining and Using TPOXX (Tecovirimat) for Treatment of Monkeypox. Available at https://www.cdc.gov/poxvirus/monkeypox/clinicians/obtaining-tecovirimat.html. Last accessed September 14, 2022.
19. Centers for Disease Control and Prevention. Monkeypox, Monkeypox and Smallpox Vaccine Guidance. Available at https://www.cdc.gov/poxvirus/monkeypox/clinicians/smallpox-vaccine.html. Last accessed September 14, 2022.
20. Centers for Disease Control and Prevention. Interim Clinical Considerations for Use of JYNNEOS and ACAM2000 Vaccines During the 2022 U.S. Monkeypox Outbreak. Available at https://www.cdc.gov/poxvirus/monkeypox/health-departments/vaccine-considerations.html. Last accessed September 14, 2022.
21. World Health Organization. Surveillance, Case Investigation, and Contact Tracing for Monkeypox: Interim Guidance, 25 August 2022. Available at https://www.who.int/publications/i/item/WHO-MPX-Surveillance-2022.3. Last accessed September 14, 2022.
22. Centers for Disease Control and Prevention. Clinical Guidance, Isolation and Prevention Practices for People with Monkeypox. Available at https://www.cdc.gov/poxvirus/monkeypox/clinicians/isolation-procedures.html. Last accessed September 14, 2022.
23. Centers for Disease Control and Prevention. Monkeypox: Prevention. Available at https://www.cdc.gov/poxvirus/monkeypox/prevention/index.html. Last accessed September 14, 2022.
24. World Health Organization. WHO Recommends New Name for Monkeypox Disease. Available at https://www.who.int/news/item/28-11-2022-who-recommends-new-name-for-monkeypox-disease. Last accessed December 12, 2022.
Mention of commercial products does not indicate endorsement.