|
| A) | Stroke | ||
| B) | Suicide | ||
| C) | Alzheimer disease | ||
| D) | Pneumonia/influenza |
| A) | The highest rate is found among White men. | ||
| B) | The number of occupational deaths is higher for men than women. | ||
| C) | The number of deaths related to motor vehicle accidents is lower for men than women. | ||
| D) | The number of deaths caused by unintentional injury among men in the United States is lower than the median for every other country around the world. |
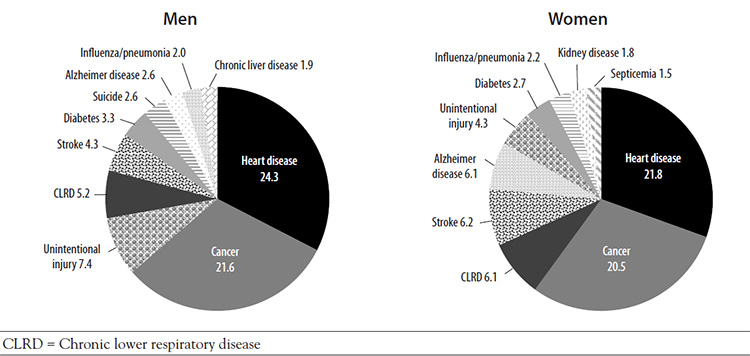
Men's predilection for risky behavior is reflected in the high rate of unintentional injury, which accounts for 7.4% of deaths among men (compared with 4.3% for women) [7,8]. There is wide variation in this rate across race/ethnicity, with much higher rates among American Indian/Alaska Native men (13.7%) and Hispanic/Latino men (11.3%) [11]. The trend of more fatal unintentional injuries among men is evident in countries around the world; an analysis of accidental deaths among men and women in 36 countries showed higher rates for men [2]. Across all age-groups, the rates were higher in the United States than the median rate for all countries. Accidental deaths are related primarily to motor vehicle injuries, violence, and occupation, and the rates in all categories are higher for men than for women. The rate of death related to motor vehicle injuries for men is slightly higher than for women (16.0 vs. 6.3 per 100,000), and the percentage of fatal unintentional firearm-related injuries deaths occur overwhelmingly more often among men (82.7%) than women (17.3%) [25]. Similarly, fatal occupational injuries occur predominantly in men (57% vs. 6%) [26].
| A) | Men are more likely than women to have screening tests. | ||
| B) | Most men seek care as soon as possible when they are sick. | ||
| C) | Men are more likely than women to lack a usual source of health care. | ||
| D) | Men are forthcoming about symptoms with their healthcare providers. |
Help- and information-seeking behavior related to male gender identity is another factor that affects men's health. In general, men are reluctant to seek health care or talk about their health because they see such help-seeking as a sign of weakness or vulnerability and a threat to their masculinity [4,35,36]. These reports are substantiated by data on utilization of healthcare resources, which indicate that men have fewer office visits to doctors or other health care professional than women; in 2018, 23.9% of men had no office visits, compared with 12.5% of women [37]. In addition, men are more likely to lack a usual source of health care (18.6% vs. 10.7%) [37]. Men have reported several reasons for not having a usual source of care, and the reasons vary among racial/ethnic populations [39]. The reason given most often is that they are seldom or never sick, and this may be related to men's perceptions of invulnerability [39,40]. Other reasons given include not finding time and not being able to take time away from work [38]. Cultural values, such as machismo, lead many Hispanic men to avoid health care until there is no other choice [40]. This may contribute to the low rate of healthcare use among Hispanic men, which is the lowest across racial/ethnic populations [40]. Other reasons for the low use of healthcare services among Hispanic men are lack of health insurance, low understanding of the healthcare system, fear of poor functional outcomes, and a low perception of the quality of the patient-clinician interaction [40]. In the Black population, men have reported to avoid healthcare services because of fears and concerns about their negative health behaviors and history [41].
| A) | the evaluation should not include a urinalysis and urine culture. | ||
| B) | the Meares-Stamey test is helpful for diagnosing chronic pelvic pain syndrome. | ||
| C) | a history of recurrent urinary tract infections is indicative of acute bacterial prostatitis. | ||
| D) | the National Institute of Health (NIH) Chronic Prostatitis Symptom Index should be completed to obtain a baseline for the severity of symptoms. |
Chronic bacterial prostatitis is distinguished from acute disease by time, being defined by persistence of symptoms for at least three months, and systemic symptoms are usually absent [58,70]. The condition should be suspected when the patient's history includes recurrent urinary tract infections, usually with the same bacterial strain [61]. The patient should complete an NIH Chronic Prostatitis Symptom Index to obtain a baseline score for the severity of symptoms [59]. This index includes questions related to three domains—pain, urinary symptoms, and quality-of-life impact—and has been shown to be a valid, reliable tool for measuring prostatitis symptoms [70,71]. Computed tomography (CT) can determine if there are structural or functional abnormalities of the urinary tract [60,61].
The diagnostic evaluation for acute or chronic bacterial prostatitis includes a urinalysis and urine culture [61,70]. When acute prostatitis is suspected, digital rectal exam should be performed gently so as not to precipitate bacteremia and sepsis. The prostate will usually be enlarged, boggy, and tender, though absence of tenderness on initial examination does not exclude the diagnosis of prostatitis. There are no standardized criteria for the diagnosis of chronic prostatitis/chronic pelvic pain syndrome [61,69]. The Meares-Stamey four-glass test was developed in the late 1960s to screen for prostatitis; the test involves collecting urine samples before and after prostatic massage, as well as collecting prostatic fluid during the massage [72]. Cultures are done on the specimens, and the presence of micro-organisms in the prostatic fluid indicates chronic prostatitis [61,72]. The accuracy and reliability of the test has not been established, and studies have shown that the test is not used often, even by urologists [61,69]. There is also a two-glass version of the test that has correlated well with the four-glass version, but that, too, is not often used [61]. The Meares-Stamey test is not helpful for diagnosing chronic pelvic pain syndrome. Men who have substantial lower urinary tract symptoms and pelvic pain may be candidates for urodynamic evaluation, as voiding dysfunction is common in such cases [61].
| A) | Trimethoprim should not be used. | ||
| B) | Pregabalin has improved symptoms. | ||
| C) | An alpha-blocker alone has provided more benefit than an alpha-blocker plus antibiotic. | ||
| D) | Fluoroquinolones have improved symptoms even when no bacterial cause has been identified. |
For chronic bacterial prostatitis, the choice of antibiotic depends on the sensitivity of the micro-organism, and the antibiotic should be one that penetrates the prostate [61]. The typical first-line treatment is a four- to six-week course of a fluoroquinolone, and treatment is usually more effective if begun soon after symptoms begin [61,70,73,74]. Trimethoprim-sulfamethoxazole may also be considered [70].
Treatment for chronic prostatitis/chronic pelvic pain syndrome is complex; evidence on the effect of traditional treatment options has been conflicting, and treatment options are often not effective in managing symptoms. The most commonly studied pharmacologic options are antibiotics, alpha-blockers, anti-inflammatory agents, steroid inhibitors, and muscle relaxants, and often, a combination of these agents provides the most effective management [74]. Antibiotics, particularly fluoroquinolones, have improved symptoms, even in some patients in whom a bacterial cause has not been identified [74]. Studies have shown that an antibiotic and an alpha-blocker is more effective than an antibiotic alone [70]. A meta-analysis showed that alpha-blockers, antibiotics, and a combination of the two all significantly improve symptoms (according to scores on the NIH Chronic Prostatitis Symptom Index), with the combination providing the greatest benefit [75]. However, another meta-analysis showed that these same agents—alone and in combination—were not associated with a statistically or clinically significant decrease in symptom scores [76]. The combination of an alpha-blocker (doxazosin) with an anti-inflammatory agent (ibuprofen) and a muscle relaxant (thiocolchicoside) led to a statistically and clinically significant reduction in the total score on the NIH Chronic Prostatitis Symptom Index in one systematic review; according to the findings of another systematic review, the three-agent combination was not superior to monotherapy [74,76]. Researchers have cautioned that publication bias may cause overestimation of the beneficial effects of alpha-blockers and that the placebo effect has been significant in many studies [75,76]. Addressing a hypothesis that the pain related to chronic prostatitis may have a neuropathic origin, pregabalin has been evaluated as a management strategy, but a systematic review found that the drug did not improve symptoms and caused side effects in a large percentage of men [77].
| A) | Asian race. | ||
| B) | increased age. | ||
| C) | a genetic mutation | ||
| D) | family history of cancer. |
The prevalence of BPH increases with age, from approximately 8% of men 31 to 40 years of age to approximately 90% of men in their 80s [80,81]. Risk factors identified in one study included increased age, prostatic volume, and peak urinary flow rate [82]. Other factors, including some that are modifiable, include obesity, diet, dyslipidemia, hypertension, alcohol use, and smoking [83]. The relative risk for BPH (and common comorbidities) may be higher for Black and Hispanic men than for White men and is thought to be related in part to genetic differences based on race/ethnicity; however, observational studies have produced variable results [81,84].
| A) | increased time to onset of disease. | ||
| B) | decreased risk for all-cause mortality. | ||
| C) | increased risk for high-grade prostate cancer. | ||
| D) | increased risk for prostate cancer-specific mortality. |
Several studies have been undertaken to determine the efficacy of chemoprevention agents and dietary supplements to reduce the risk of prostate cancer. The chemoprevention agents evaluated belong to the class of 5-alpha reductase inhibitors, a class of drugs approved for the treatment of BPH. One drug in this class, finasteride, was evaluated in the first large-scale chemoprevention study, the Prostate Cancer Prevention Trial (PCPT), a seven-year study involving nearly 19,000 men 55 years of age or older. In that study, finasteride significantly reduced the prevalence of prostate cancer (18% vs. 24% for the placebo group) [98]. Dutasteride was shown to decrease the risk of prostate cancer in the REDUCE trial, and extended follow-up indicated a low rate of new prostate cancer diagnoses [99,100]. The initial results of the PCPT and REDUCE trials led the American Society of Clinical Oncology (ASCO) and the AUA to develop a joint guideline recommending finasteride and dutasteride for the prevention of prostate cancer [90]. However, reanalysis of the results of the trials showed that the risk for high-grade prostate cancer was increased and the reduction in prostate cancer risk was seen primarily for less fatal subtypes of prostate cancer that are often not treated [100,101]. In 2011, the FDA decided against approving the two drugs for the prevention of prostate cancer, noting that the risk-benefit profile is not favorable for chemoprevention [91,101,102]. As stated earlier, the FDA revised the labels of all 5-alpha reductase inhibitors to note the increased risk of higher-grade prostate cancer associated with the drugs [92]. The ASCO/AUA guideline was withdrawn, and experts have called for more research to determine whether 5-alpha reductase inhibitors have a role in the prevention of prostate cancer [101,102,103].
| A) | lower mortality rates. | ||
| B) | decreased need for biopsy. | ||
| C) | diagnosis at an earlier stage. | ||
| D) | higher prevalence of definitive disease. |
There is no question that available screening methods and enhanced awareness has led to an increased number of men in whom prostate cancer is diagnosed at an earlier stage. The primary benefit of screening is a lower stage and grade of cancer at the time of diagnosis, and the high rate of localized disease at the time of diagnosis (92% to 96%) reflects, in part, the increased number of cancers that are detected earlier through screening [102,108,109]. Despite this benefit, an effect of screening on mortality has not been clearly demonstrated. After 13 years of follow-up in the National Cancer Institute's Prostate, Lung, Colon, and Ovary (PLCO) trial, there was no benefit of annual screening on mortality [110]. A meta-analysis (five randomized controlled trials) similarly demonstrated no effect of screening on prostate cancer-specific or overall mortality [111]. However, data from the European Randomized Study of Screening for Prostate Cancer demonstrated that screening reduced the risk for prostate cancer death by 7% to 9% per year [112].
| A) | Radiation therapy | ||
| B) | Active surveillance | ||
| C) | Radical prostatectomy | ||
| D) | Androgen deprivation therapy |
The NCCN Panel recommends active surveillance for all men with very-low-risk prostate cancer and a life expectancy of less than 20 years and believes that surveillance should be considered for men with very-low-risk prostate cancer and a life expectancy of 20 years or more [126]. In addition, the Panel recommends active surveillance for all men with low- and favorable intermediate-risk prostate cancer and a life expectancy of less than 20 years and believes that it should be considered for men with low- and favorable intermediate-risk and a life expectancy of 10 years or more [126]. With active surveillance, recommended monitoring is measurement of a PSA level no more than every 6 months, unless clinically indicated, and physical exam with DRE every 12 months [126]. An increase in PSA should prompt re-testing as transient PSA elevations are common; serial PSA increases, new DRE abnormalities, or other concerns for clinical progression should prompt re-evaluation with prostate MRI and possible prostate biopsy [126,358].
| A) | brachytherapy. | ||
| B) | chemotherapy. | ||
| C) | radical prostatectomy. | ||
| D) | androgen deprivation therapy. |
Both NCCN and ASCO recommend ADT as initial treatment for metastatic prostate cancer [126,155]. Researchers have evaluated the timing of ADT—early (before symptoms occur) or delayed—and early therapy has provided no overall survival benefit and only a modest decrease in risk for prostate cancer-specific mortality; because of this, the ASCO guideline does not make a recommendation for early ADT [155]. Several studies have demonstrated that intermittent ADT is as effective as continuous ADT for metastatic or locally advanced disease, with better quality of life and fewer side effects [156,157,158].
| A) | urinary retention. | ||
| B) | unilateral tenderness. | ||
| C) | pain with extended standing. | ||
| D) | sudden onset of pain in both testicles. |
Men with acute epididymitis usually present with unilateral pain and tenderness in the testicle [173]. Additional symptoms include dysuria, urinary frequency or urgency, and symptoms related to the source of infection (e.g., fever, chills, or pain). Urinalysis and urine culture should be done to determine the presence of infection [175,176].
| A) | more common in infertile men. | ||
| B) | a source of substantial unilateral pain. | ||
| C) | more pronounced when the patient is recumbent. | ||
| D) | associated with a hardness of the testes in older men. |
A varicocele is a dilated, tortuous inflammation of the veins of the spermatic cord above the testicle. A prevailing thought has been that the superior mesenteric artery compresses the left renal vein over the aorta, also known as the "nutcracker effect" [178]. This theory has been confirmed by studies that have shown that varicoceles are less common in obese men [178,179]. It has also been suggested that the condition is caused by damage to the contractile mechanism of the smooth muscle organization of spermatic veins [180]. As a result of anatomic differences, the condition is more common in the left testicle, but advances in imaging have led to reports of high rates of bilaterality [181]. Varicocele can cause discomfort in the scrotal area, but usually the condition is asymptomatic [165].
The frequency of varicocele among adolescents and young adults is approximately 15% to 20%, and the rate is higher among men who have some level of infertility, with reports of 77% and 81% in some studies [181,182]. A study of older men (mean age: 60.7 years) demonstrated a prevalence of 42% [183].
Varicoceles vary in size, and large ones can be identified through physical examination alone. Varicoceles can have an adverse effect on spermatogenesis, and infertility has been associated with varicoceles that can be palpated [182]. The most significant finding is a feeling of a "bag of worms" when the scrotum is palpated [165,182]. The varicocele may disappear or be substantially reduced when the patient is recumbent [182]. Smaller varicoceles can be detected by asking the patient to perform the Valsalva maneuver in the standing position [182]. In older men (at least 60 years of age), varicoceles have been associated with significantly smaller and soft testes [183]. Color Doppler ultrasonography is the diagnostic procedure of choice when the findings of the clinical examination are inconclusive [182].
| A) | AFP level. | ||
| B) | LDH level. | ||
| C) | beta-hCG level. | ||
| D) | beta-hCG level and a normal AFP level. |
According to the NCCN guideline for the treatment of testicular cancer, testicular ultrasonography is optional if a diagnosis is obvious from the physical examination, but the guideline notes that this diagnostic test is usually done to define the lesion [177]. Both the NCCN and ASCO recommend measuring serum levels of alpha-fetoprotein (AFP), human chorionic gonadotropin (beta-hCG), and lactate dehydrogenase (LDH) to help determine if the testicular mass is a germ cell tumor and, if so, whether it is a seminoma or a nonseminoma [177,194]. A nonseminoma is associated with an elevated AFP level; in contrast, an elevated level of beta-hCG, with a normal AFP level, usually indicates a seminoma [177]. Additional evaluation should include a chest x-ray and CT of the abdomen and pelvis to determine if lymph nodes are involved [177]. If metastatic disease is suspected, further imaging studies, such as bone scan, magnetic resonance imaging, or positron emission tomography, may be necessary. Open biopsy is not usually performed [177].
| A) | hearing loss. | ||
| B) | oligospermia. | ||
| C) | erectile dysfunction. | ||
| D) | secondary leukemias. |
The follow-up evaluation plays an important role in assessing for the long-term effects of treatment. The primary effect of chemotherapy is oligospermia, but sperm production can be recovered [195,196]. A population-based study found that 70% of testicular cancer survivors fathered children [197]. Secondary acute leukemias have been reported to develop after chemotherapy and radiation therapy, and other consequences of platinum-based chemotherapy include hearing deficits and impaired renal function [198,199]. Melanomas and cancers at many sites have been associated with radiation therapy, occurring 10 years or more after treatment [198]. Lastly, the risk of cardiac events has been increased for testicular cancer survivors who had been treated with radiation therapy and/or chemotherapy [200].
| A) | Lumpectomy is rarely performed. | ||
| B) | The BRCA2 mutation is found in most cases. | ||
| C) | Adjuvant hormone therapy has a limited role in treatment. | ||
| D) | Sentinel lymph node biopsy has not been found to be effective. |
BRCA2 mutation is found in approximately 4% to 16% of men with breast cancer [203].
A painless subareolar lump or swelling is the most common presenting symptom, occurring in approximately 85% of men with breast cancer [201,204]. Other common symptoms are nipple retraction, localized pain, or nipple ulceration, bleeding, or discharge. About 1% to 2% of men will have no symptoms [201,204]. In diagnosing male breast cancer, the primary consideration is to distinguish cancer from gynecomastia, which is present in about 30% of healthy men [202].
The approach to the diagnostic evaluation of male breast cancer is the same as for female breast cancer. A history and physical examination will help determine potential risk factors and identify the clinical features. Mammography has good sensitivity and specificity, and ultrasonography may be useful, especially for detecting involvement of the lymph nodes [202]. Biopsy is essential for elucidating the pathologic characteristics. In male breast cancers, the overexpression of estrogen receptor and progesterone receptors is likely [203,205].
As noted, data on male breast cancer are limited, and recommendations for treatment have been extrapolated from the literature on female breast cancer and from small series of men with the disease. Modified radical mastectomy is used most often, with lumpectomy rarely performed [203]. Sentinel node biopsy has also been effective in men [206,207]. Adjuvant radiation therapy has been associated with a lower local recurrence rate and a higher survival rate [202,203]. Adjuvant chemotherapy has been carried out according to guidelines for women at high risk for recurrence. Adjuvant hormone therapy has a clear role in the treatment of men with hormone receptor-positive cancer, with reductions in recurrence and death [204,208]. In addition, tamoxifen has led to a 50% response rate for metastatic breast cancer [202].
| A) | Obesity | ||
| B) | Depression | ||
| C) | History of smoking | ||
| D) | Cardiovascular disease |
Erectile dysfunction has been reported to be more common among men with comorbidities; independent risk factors include age, diabetes, metabolic syndrome, cardiovascular disease, obesity, and sedentary lifestyle [214,234,235]. Among men with no known cardiovascular disease, erectile dysfunction has preceded coronary artery disease, stroke, and peripheral artery disease by an average of three years (range: two to five years) [236]. In addition, a meta-analysis (14 cohort studies; 92,757 men) showed that erectile dysfunction was an independent risk factor for cardiovascular and cerebrovascular events [237]. Other risk factors for erectile dysfunction include hormone disorders, neurologic conditions, psychologic disorders, history of surgery or radiation in the pelvic region, use of illicit drugs, and some prescription drugs (most notably, antihypertension agents) [238]. Encouraging men with these risk factors to modify their lifestyle and/or treating comorbidities may help reduce the risk of erectile dysfunction [239].
| A) | serum half-life. | ||
| B) | side effect profile. | ||
| C) | duration of action. | ||
| D) | time to maximum serum level. |
After treatment of erectile dysfunction is initiated, referral to a mental health professional should be considered to promote treatment adherence, reduce performance anxiety, and integrate therapies into a sexual relationship [355]. Both the AUA and the ACP recommend oral phosphodiesterase-5 inhibitors as first-line pharmacotherapy for erectile dysfunction in men for whom this class of drugs is not contraindicated [230,231,355]. Four drugs in the class have been approved for use in the treatment of erectile dysfunction: sildenafil (Viagra), tadalafil (Cialis), vardenafil (Levitra), and avanafil (Stendra, Spedra). Sildenafil and vardenafil differ from tadalafil with respect to the time to maximum serum level (1 hour vs. 2 hours) and serum half-life (4 hours vs. 18 hours) [230]. Furthermore, the duration of action is longest for tadalafil (up to 36 hours) [240]. The inhibitory effect of these drugs causes vascular smooth muscle relaxation in the corpus cavernosum, resulting in increased erection hardness and prolonged duration in men with erectile dysfunction who have sufficient intact vasculature [355].
Data from multiple trials and systematic reviews have demonstrated similar efficacy for phosphodiesterase-5 inhibitors in treating erectile dysfunction, particularly for sildenafil, tadalafil, and vardenafil [355]. Each of these drugs substantially improves erectile function and successful sexual intercourse compared with placebo [231]. Relative efficacy is less clear for avanafil because published comparative studies are limited. The ACP notes that there is insufficient evidence for recommending one drug over another and suggests that the choice be made according to the preferences of an individual patient with respect to ease of use, cost, and the adverse effects profile [231]. One systematic review and meta-analysis found evidence that tadalafil is the most effective agent, followed by vardenafil, with no major differences in the safety profile of any of the phosphodiesterase-5 inhibitors [241].
The side effects of all four drugs are similar, with headache, dyspepsia, facial flushing, nasal congestion, and visual disturbances being the most common events [230,240,242]. The FDA has issued two mandates to revise labeling of these agents. In 2005, the agency required labels for sildenafil, tadalafil, and vardenafil to reflect the possibility of sudden vision loss after taking the drugs for a period of time [243]. The alert was associated with several case reports suggesting a temporal association between use of one of the drugs and nonarteritic anterior ischemic optical neuropathy (NAION), a rare disorder characterized by sudden loss of vision in one eye [243,355]. However, subsequent studies showed that the risk of NAION was similar among men who were and were not taking a phosphodiesterase-5 inhibitor [244,245]. Risk factors for spontaneous NAION include older age, White race, small optic discs with low cup-to-disc ratio, and vascular disease, leading some investigators to suggest an examination of the fundus be performed on men who may be at higher risk for NAION before a phosphodiesterase-5 inhibitor is prescribed [243].
| A) | equivalent to menopause in women. | ||
| B) | well defined by a level of testosterone. | ||
| C) | similar to hypogonadism in younger male individuals. | ||
| D) | associated with a loss of sexual satisfaction and overall well-being. |
Late-onset hypogonadism is distinct from hypogonadism in younger male individuals. For boys and young men, hypogonadism is related to testicular failure and is usually associated with a congenital abnormality, most often Klinefelter syndrome [251]. In older men with hypogonadism, testosterone levels are rarely as low as the levels in young men with primary hypogonadism [251].
Several important questions about late-onset hypogonadism remain unanswered [252,253]:
It is unclear whether the symptoms are caused by a reduction in testosterone or are a result of the normal physiologic process of aging.
There is no consistent level of testosterone to define hypogonadism, and there is confusion about what testosterone levels should be measured.
There is ongoing debate about the risk-benefit ratio of testosterone therapy for older men.
| A) | is correctable in most cases. | ||
| B) | is not affected by prescription medications. | ||
| C) | is the only cause in most cases of infertile couples. | ||
| D) | affects men younger than 25 years of age twice as often as older men. |
Infertility is clinically defined as the inability to conceive after one year of unprotected intercourse [264]. Approximately 15% of couples are unable to conceive after one year of unprotected intercourse. A male factor is the only cause in approximately 20% of infertile couples and is a contributing factor in another 20% to 40% [264]. Fertility declines with age, and research has shown that men older than 35 years of age are twice as likely to be infertile as men younger than 25 years of age [265,266]. Approximately 15% of infertile men have azoospermia, the complete absence of sperm in the ejaculate [267].
More than half of male infertility or subfertility is potentially correctable; often, the cause is unknown. The causes, both correctable and uncorrectable, include [264,268]:
Varicocele
Obstruction of a duct (epididymal, vasal, or ejaculatory)
Ejaculatory dysfunction
Testicular atrophy
Hypogonadotropic hypogonadism
Infection
Side effects of medication
Environmental toxins
Bilateral cryptorchidism
Genetic abnormality (Y chromosome microdeletion)
Congenital absence of vas deferens
| A) | chlamydia. | ||
| B) | hepatitis B. | ||
| C) | herpes simplex virus 2. | ||
| D) | human papillomavirus. |
The CDC recommends that all individuals who are evaluated for gonorrhea should also be evaluated for chlamydia, syphilis, and HIV infection [173]. In one study of more than 3,800 men and women, approximately 10% to 30% of individuals with gonorrhea had concomitant infection with chlamydia [290]. The typical lesions of genital HSV-2 in men appear on or around the penis and are first noted as either a single or multiple erythematosus macular lesion(s). However, these lesions are absent in many infected individuals [173]. Viral culture is the preferred test for the diagnosis of HSV-2, but it requires two to seven days for results. The sensitivity of viral culture depends on the quality of the sample and the time at which the sample is obtained; sensitivity declines as the lesion begins to heal. A PCR test is available and is suggested by the CDC for analysis of cerebrospinal fluid when central nervous system disease is suspected [173]. Type-specific serologic tests are available as laboratory assays and point-of-care tests [173]. These tests have varying degrees of sensitivity for the detection of the HSV-2 antibody (80% to 90%) and specificity of at least 96% [173].
| A) | Acyclovir | ||
| B) | Benzathine penicillin | ||
| C) | Ceftriaxone and doxycycline | ||
| D) | Azithromycin and penicillin G |
TREATMENT OF CHLAMYDIA, SYPHILIS, AND GONORRHEA AS RECOMMENDED BY THE CENTERS FOR DISEASE CONTROL AND PREVENTION
| Infection | Recommended Treatment | Notes | |||||
|---|---|---|---|---|---|---|---|
| Chlamydia |
| A meta-analysis showed treatment failure among men was higher for azithromycin than for doxycycline. | |||||
| Gonorrhea |
|
| |||||
| Primary and secondary syphilis | Benzathine penicillin G 2.4 million units IM (single dose) |
|
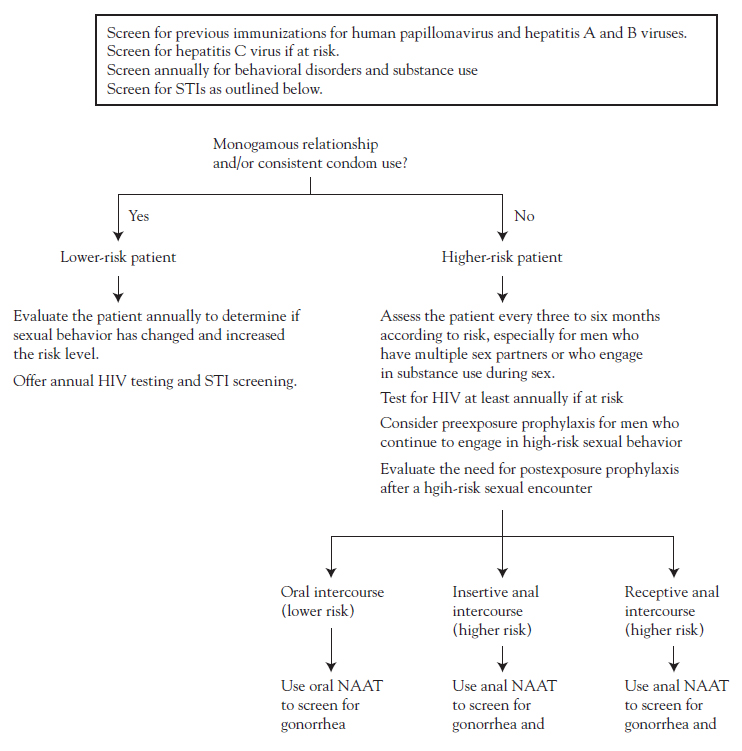
| A) | High-risk patients should be assessed yearly. | ||
| B) | Annual HIV screening should not be considered for low-risk men. | ||
| C) | Hepatitis A and B immunization should be assessed in high-risk patients only. | ||
| D) | Anal NAAT should be considered for men who have receptive anal intercourse. |
| A) | The misuse of illicit drugs is expected to decrease as the general population ages. | ||
| B) | The rate of alcohol misuse is higher among younger women than among younger men. | ||
| C) | Men are less likely than women to have psychosocial problems related to substance misuse. | ||
| D) | Men older than 65 years are much more likely to be "problem" drinkers than women in that age group. |
As noted, substance misuse is higher among men than among women in all age categories, and men are more likely to have psychosocial problems related to the misuse [28,307]. Although the rate of alcohol misuse is highest among younger men, men older than 65 years of age are of special concern because they are much more likely than women to be "problem" drinkers and to misuse a wide range of illicit as well as prescription drugs [307]. As the general population ages, the misuse of illicit drugs is expected to increase [314]. Adding to this problem is the low rate of screening for alcohol misuse in the older population and the secrecy of many men about drug use [314,315].
| A) | pharmacologic therapy alone. | ||
| B) | cognitive behavioral therapy alone. | ||
| C) | interpersonal psychotherapy alone. | ||
| D) | psychotherapy and pharmacologic therapy. |
The treatment approach will depend on the severity of symptoms and the patient's preference. In general, a combination of psychotherapy and pharmacologic management provides the best results for most men [328,335]. Potential psychotherapy approaches include cognitive behavior therapy and interpersonal psychotherapy [300,307,328]. First-line pharmacologic treatment involves the use of selective serotonin reuptake inhibitors, such as paroxetine, sertraline, and fluoxetine [307]. This treatment approach has efficacy rates of 30% to 70% [328]. Clinicians should emphasize the importance of taking the medication as prescribed, as it may be two to four weeks before a benefit is evident [328]. Depression that is associated with chronic illness is often seen as an inevitable consequence of the disease, but the depression should be treated. Frequently, the treatment improves the overall outcome [335].
| A) | Health fairs | ||
| B) | Support groups | ||
| C) | Short video clips | ||
| D) | Pamphlets emphasizing the importance of prevention |
As a result of men's reluctance to seek help, educational strategies that provide anonymity may be particularly well-suited for them [45,339]. Print resources should be distributed through a variety of venues that men frequent, such as the workplace, schools, religious organizations, sports arenas, men's organizations or clubs, pubs, supermarkets, car and motorbike dealerships, and barbershops [45,339,340]. In addition, digital media may be effective, especially for younger men. A study showed that 90-second educational video clips on men's health, sent by e-mail, were well-received [341].