Study Points
- Back to Course Home
- Participation Instructions
- Review the course material online or in print.
- Complete the course evaluation.
- Review your Transcript to view and print your Certificate of Completion. Your date of completion will be the date (Pacific Time) the course was electronically submitted for credit, with no exceptions. Partial credit is not available.
Study Points
Click on any objective to view test questions.
- Describe the underlying pathophysiology of pain.
- Outline the different types of pain.
- Discuss the mechanism of action and clinical use of opioids in the management of pain.
- Compare and contrast other analgesic agents that can be used in a multimodal approach to pain management, including nonsteroidal anti-inflammatory drugs (NSAIDs), antidepressants, and local anesthetics.
- Analyze approaches to multimodal pharmacotherapy for pain management.
The function of free nerve endings (FNEs) is to transmit information regarding
Click to ReviewTYPES OF SENSORY RECEPTORS
Type Function Location Free nerve ending Transmit pain and temperature Skin, periosteum, arterial walls, joint surfaces Pacinian (lamellar) corpuscle Pressure Skin Meissner (tactile) corpuscle Touch Skin Muscle spindle Stretch and pressure Skeletal muscle Golgi tendon apparatus Stretch and pressure Tendons Kinesthetic receptor Three-dimensional location (proprioception) Joints Action potentials are
Click to ReviewAction potentials are changes in polarity along a nerve based on ion flow into and out of the nerve cell. As the action potential travels down the length of the cell, it will end at a point in the nervous system that results in some form of output, either physical (muscle movement) or experiential (pain).Figure 2 shows some of the details of an action potential and provides an extended explanation of their formation. Of particular importance is the quantity of ions moving at any specific time. The primary ions moving after stimulation and reaching threshold are Na+ (sodium, into the cell), K+ (potassium, out of the cell), and Cl- (chloride, into the cell). After the nerve has fired, the sodium/potassium adenosine triphosphate (ATP)-ase pump works to move sodium out of the cell and potassium back into the cell. A pump is needed because the ions are moving against their gradients, and energy is required in the form of ATP to power the pump [7].
What are the two primary types of nerves that carry pain data elicited by stimulation of an FNE?
Click to ReviewThere are two primary types of nerves that carry pain data elicited by stimulation of an FNE: type Aδ or myelinated (fast) nerve fibers and type C or unmyelinated (slow) nerve fibers [5,8]. Myelinated fibers are insulated with Schwann cells, but with gaps (nodes of Ranvier) in which the nerve fiber is exposed to the environment of the extracellular fluid. The myelinated fibers are also referred to as fast fibers because the action potentials can skip between the nodes of Ranvier in a process called saltatory conduction (rather than traveling the entire length of the axon). Sharp or acute pain, especially from traumatic injury, is usually processed in this fashion.
At what point does a first-order neuron synapse with a second-order neuron?
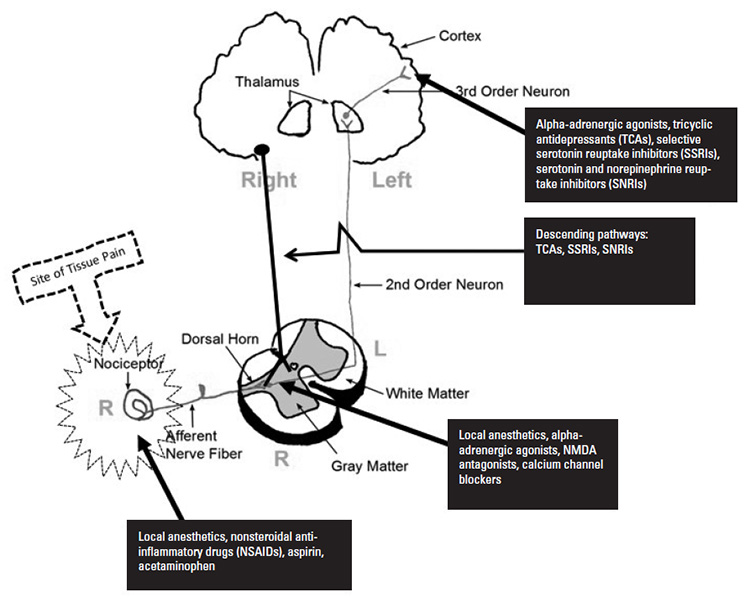
Click to ReviewPain and other impulses originate in the peripheral nervous system (PNS), enter the dorsal horn of the vertebra, and then ascend to the brain along the spinothalamic tract. This is a three-neuron pathway containing first-, second-, and third-order neurons. In Figure 4, the spinothalamic tract can be traced from the primary afferent nerve (receiving the pain signals at the site of injury) to the spinal cord, entering via the dorsal root of the cord. At this point, the first-order neuron synapses with a second-order neuron. Upon entry into the cord, the second-order neuron crosses from the right to the left (or left to right, if it enters the left dorsal root). This is referred to as decussation. The second-order neuron then rises up the cord in either the anterior or later spinothalamic tract, synapsing with a third-order neuron in the thalamus. This neuron leads to the sensory cortex in the brain, which in turn interprets the exact location and degree of pain.
Glutamate
Click to ReviewSUBSTANCES AFFECTING THE TRANSMISSION OF IMPULSES IN FREE NERVE ENDINGS AND SOMATIC NERVES
Substance Description Bradykinin Bradykinin is a vasodilator that increases capillary permeability, increases migration of white blood cells, and increases free radicals in inflamed tissue and significantly excites pain receptors. Calcitonin gene-related peptide (CGRP) Stimulation of the free nerve endings results in the release of CGRP from the neuron, sensitizing it to stimuli and making the neuron hyperactive. Norepinephrine Pain stimulates the sympathetic nervous system, leading to the release of norepinephrine, which has an excitatory effect on the neuron. Glutamate Glutamate is an endogenous and highly excitatory neurotransmitter that binds at both the NMDA and AMPA receptors to excite the neuron and facilitate pain transmission. Histamine A ubiquitous substance throughout the body, histamine is released by mast cells and binds with excitatory receptors on the neurons and other cells. Tachykinin Tachykinins are a broad family of neuropeptides, including substance P, neurokinin A, and neurokinin B, released in response to pain or inflammation. They bind with neurokinin receptors, resulting in increasing excitatory stimulation of the neuron. Serotonin (5-HT) During inflammation, 5-HT is released from platelets in the area of injury. In turn, these bind with 5-HT2A and 5-HT3 receptors, resulting in excitation of the nerve. Prostaglandin One of the most crucial substances in pain management, prostaglandin sensitizes all aspects of excitatory phenomena in neurons. They are produced from the cell's arachidonic acid supply via the cyclo-oxygenase and lipoxygenase pathways. Cytokine Cytokines increase synaptic excitatory transmission in neurons and are represented by such substances as TNF and interleukins (e.g., IL-1b, IL-6). AMPA = α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid, NMDA = N-methyl-D-aspartate, TNF = tumor necrosis factor. The projection of the neurons into what area of the brain accounts for the suffering aspect of pain, where the sensation is overlaid with an emotional experience?
Click to ReviewThe thalamus also has neuronal branches that help to stimulate the reticular activating system, the portion of the brain responsible for sleep and waking [5]. The thalamus has numerous projections into other areas of the brain, including the prefrontal cortex and the amygdala, the latter of which is part of the limbic system [16,17]. The projections of the neurons into the limbic system account for the suffering aspect of pain, where the sensation is overlaid with an emotional experience. As pain is important in preventing homeostasis damage, including an emotional response to pain (in addition to a sensory response) helps ensure the person experiencing pain will avoid the stimulus that led to the pain.
Hyperalgesia is the
Click to ReviewPain pathways stimulate many areas of the brain. The brain responds by the release of many neurotransmitters and other hormones to provide a systemic response [10]. As discussed, pain impulses activate the amygdala, which triggers a sympathetic nervous system response, sometimes referred to as the "fight-or-flight" response. The release of norepinephrine and epinephrine results in, among other things, tachycardia, hypertension, and elevated blood glucose levels. Additionally, the local response to the stimulus produces the release of local neurotransmitters, such as substance P, glutamate, CGRP, and brain-derived neurotrophic factor (BDNF) [10,11]. Of perhaps greater concern is the release of cytokines, which results in a profound inflammatory response. The inflammatory response is usually highlighted by hyperalgesia (exaggerated painful response to a painful stimulus) and allodynia (painful response from a non-pain-inducing stimulus). Take the example of a minor sunburn. If the skin is reddened and inflamed, a pat on the back becomes inordinately painful (hyperalgesia) and simply wearing a shirt may be intolerable (allodynia). In addition to these responses, untreated acute pain may lead to the expression of additional FNEs and nociceptors.
Nociceptive pain is
Click to ReviewNociceptive pain is a physiologic response to tissue injury, the perception that arises from intense stimulation of specialized peripheral sensory neurons (nociceptors) that respond only to noxious (pain) stimuli. Nociceptive pain is subgrouped by location of involved tissues into somatic pain (muscle or connective tissue) and visceral pain (visceral structures). Nociceptive pain is considered adaptive during tissue healing but maladaptive and pathologic when it persists after healing has occurred. For example, inflammatory pain occurs in response to tissue injury or infection that activates peripheral nociceptors and initiates the immune response. While the resultant production and recruitment of pro-inflammatory mediators to the injury site may serve to perpetuate discomfort, it also facilitates tissue repair; thus, this is considered an adaptive pain mechanism [37,38,39].
Which of the following is an example of a centralized pain syndrome?
Click to ReviewNociplastic pain results from alterations of nociceptive processing, such as heightened central excitability and/or diminished central inhibition (i.e., central sensitization). Nociplastic pain is typically chronic and more widespread than nociceptive pain. The mechanism is poorly understood and is regarded as strictly pathologic as it lacks any evident adaptive function. Nociplastic pain can occur independently of peripheral nociceptor activity; however, some conditions involve both nociceptive and nociplastic pain mechanisms (e.g., peripheral and central sensitization) to varying degrees along a continuum. Centralized pain syndromes include conditions such as fibromyalgia, low back pain, and carpal tunnel syndrome [37,38,39,40].
Which of the following drug classes acts on descending pain pathways?
The three primary opioid receptor types are
Click to ReviewNaturally occurring opioid compounds are produced in plants (e.g., opium, morphine) and in the body (the endogenous opioids). Endogenous opioids are peptides that bind opioid receptors, function as neurotransmitters, and help regulate analgesia, hormone secretion, thermoregulation, and cardiovascular function. The three primary endogenous opioid peptide families are the endorphins, enkephalins, and dynorphins, and the three primary opioid receptor types are mu, kappa, and delta [44,45]. A quick overview of this complex pain modulation system is helpful in understanding how opioid analgesics work.
Opioid antagonists are FDA-approved for the treatment of
Click to ReviewIn addition to opioid-induced constipation, opioid antagonists are U.S. Food and Drug Administration (FDA)-approved for the treatment of alcohol and opioid use disorder (naltrexone 50–100 mg/day oral) and opioid overdose (naloxone 0.4–1.0 mg/dose IV or IM). In pain medicine, the dose ranges of naltrexone and naloxone are substantially lower. Of the two, naltrexone is much more widely used, and published pain medicine studies have used dose ranges of 1–5 mg (termed "low-dose") or <1 mg in microgram amounts (termed "ultra-low-dose") [65]. For example, case studies have reported dramatic improvement in refractory pain with intrathecal administration of an opioid agonist combined with ultra-low-dose naloxone in the low nanogram range [68].
NSAIDs alleviate pain by
Click to ReviewNSAIDs alleviate pain by inhibiting the conversion of arachidonic acid to prostaglandins catalyzed by COX isozymes. Nonselective NSAIDs inhibit COX-1 and COX-2 and include ibuprofen, aspirin, and naproxen. The nonselective action inhibits the formation of both gastroprotective-mediating prostaglandins and pain-promoting prostaglandins, increasing the risk of serious toxicities such as GI ulceration and bleeding. This prompted the development of selective COX-2 inhibitors, which produce fewer GI side effects but are linked with an increased risk of cardio-renal morbidities [71]. To mitigate risk of GI adverse events, proton pump inhibitors are recommended for use in some patients using NSAIDs [72].
Diclofenac is available in all of the following routes, EXCEPT:
Click to ReviewCOMMONLY USED NONSTEROIDAL ANTI-INFLAMMATORY DRUGS (NSAIDs) AND ACETAMINOPHEN
Drug Route(s) Meloxicam (Anjeso) IV, PO Ketorolac (Toradol) PO, IM, IV, eye drops, nasal spray Ibuprofen (Motrin, Advil) PO, IV Diclofenac (Cataflam, Voltaren) PO, IM, IV, eye drops, topical gel Naproxen (Aleve, Anaprox) PO Celecoxib (Celebrex, Elyxyb) PO Aspirin PO Acetaminophen (Tylenol) PO, IV, rectal The maximum dose of lidocaine administered with epinephrine is
Click to ReviewMAXIMUM DOSES OF LOCAL ANESTHETICa
Local Anesthetic Ester or Amide Maximum Dose Per Kilogram Plain Maximum Dose Plainb Maximum Dose Per Kilogram with Epinephrine Maximum Dose with Epinephrineb Bupivacaine (Marcaine) Amide 2 mg/kg 175 mg 3 mg/kg 225 mg Levobupivacaine (Chirocaine) Amide 2 mg/kg 200 mg 3 mg/kg 225 mg Lidocaine (Xylocaine) Amide 5 mg/kg 350 mg 7 mg/kg 500 mg Mepivacaine (Carbocaine) Amide 5 mg/kg 350 mg 7 mg/kg 500 mg Ropivacaine (Naropin) Amide 3 mg/kg 200 mg 3 mg/kg 500 mg Prilocaine (Citanest) Amide 6 mg/kg 400 mg 8 mg/kg 250 mg Procaine (Novocaine) Ester 7 mg/kg 1,000 mg 10 mg/kg 600 mg Tetracaine (Amethocaine) Ester 0.2 mg/kg 20 mg N/A 1,000 mg aDoses vary by country and institution, familiarize yourself with your local policies regarding maximum doses before administering bIf administering a local anesthetic to a large patient, stop at the maximum dose, even if the mg/kg dose would exceed it. Which of the following statements regarding calcium channel blockers is TRUE?
Click to ReviewThe gabapentinoids, gabapentin and pregabalin, are widely used in the management of both postoperative and chronic pain relief. Their names may give the impression they interact with gamma-amino butyric acid (GABA), but this is not the case [86,87]. Gabapentin and pregabalin are anticonvulsants that are also effective in a wide range of neuropathic pain conditions. Their mechanism of action involves selective binding to and blockade of the α2δ1 subunit of voltage-gated calcium channel in various brain regions and the superficial dorsal spine. This inhibits the release of glutamate, norepinephrine, and substance P to decrease spinal cord levels of neurotransmitters and neuropeptides [76,88,89]. The binding affinity of pregabalin for the calcium channel α2δ1 subunit is six times greater than gabapentin, which is reflected in the greater efficacy of pregabalin at lower doses. Because gabapentin possesses a shorter half-life and nonlinear absorption, pregabalin is easier to titrate and better tolerated [89].
All of the following are alpha-adrenergic agonists, EXCEPT:
Click to ReviewWhile more commonly associated with the autonomic nervous system and its functions, alpha-adrenergic agonists can also function in the relief of pain, as well as decreasing the sympathetic side effects which accompany pain, including hypertension and tachycardia. Antinociceptive activity of the α-2 adrenoceptor agonists clonidine and tizanidine includes modulating dorsal horn neuron function and norepinephrine and 5-HT release, potentiating mu-opioid receptors, and decreasing neuron excitability through calcium channel modulation [92]. Clonidine is available as a transdermal patch for use in neuropathic pain states. Local use enhances release of endogenous enkephalin-like substances. Intrathecal or epidural administration with opioids and/or local anesthetics is favored in treating neuropathic pain because the synergistic effect improves pain control. Tizanidine is used as a muscle relaxant and antispasticity agent; its use in the management of musculoskeletal pain is off label [76,79].
Dexmedetomidine was originally approved as a short-term sedative analgesic for mechanically ventilated patients in the intensive care unit [93]. Dexmedetomidine is far more selective as an alpha-adrenergic agonist and has the same central action around the locus coeruleus [93]. As time passed since its introduction, the use of dexmedetomidine has increased, especially among patients with comorbidities (e.g., heart and vascular disease, morbid obesity). Its cardiovascular stability, along with its minimal effect on respiratory drive after the infusion is terminated, have made this agent popular in both the intensive care unit and the operating room. Aside from its use as a sedative or aesthetic agent, use of dexmedetomidine has been explored in patients with refractory end-of-life pain. In a case study, a male patient, 58 years of age, with chronic pancreatitis secondary to alcoholism reported inadequate pain relief despite receiving a combination of oxycodone, nortriptyline, and lorazepam. Increased inpatient intravenous opioids and ketamine still brought the patient no relief, and dexmedetomidine was attempted as a last resort. An infusion of dexmedetomidine brought the patient's pain under greater control, to the extent that he was able to sit in a recliner and visit with family [94]. Based on this and other reports, dexmedetomidine is being explored as a possible option in palliative care.
The mechanism of action of ketamine primarily involves
Click to ReviewKetamine is a phencyclidine anesthetic given parenterally, neuraxially, nasally, transdermally or orally in subanesthetic doses to alleviate a variety of pain conditions, including severe acute pain, chronic or neuropathic pain, and opioid tolerance [79]. The mechanism of analgesic effect primarily involves NMDA receptor inhibition. Thus, patients with NMDA-mediated central sensitization are likely to realize significant benefit from treatment with ketamine. Ketamine also has activity on nicotinic, muscarinic, and opioid receptors and exerts both anti-nociceptive and anti-hyperalgesic effects, with the latter produced at lower dose ranges [98].
Which of the following is NOT a serotonergic and noradrenergic re-uptake inhibitor (SNRI)?
Click to ReviewThe dual serotonergic and noradrenergic re-uptake inhibitors (SNRIs) duloxetine, venlafaxine, and milnacipran are widely used in the treatment of neuropathic pain conditions. Duloxetine is used in painful diabetic neuropathy, with demonstrated efficacy at 60–120 mg/day. Venlafaxine behaves like a SSRI at doses of ≤150 mg/day and like an SNRI at doses >150 mg/day; a dose ≥150 mg/day is often necessary to achieve pain control [76]. Of the three available SNRIs, milnacipran has the greatest affinity for norepinephrine, duloxetine has the greatest potency in blocking serotonin, and venlafaxine selectively binds to the serotonin but not the norepinephrine transporter [115].
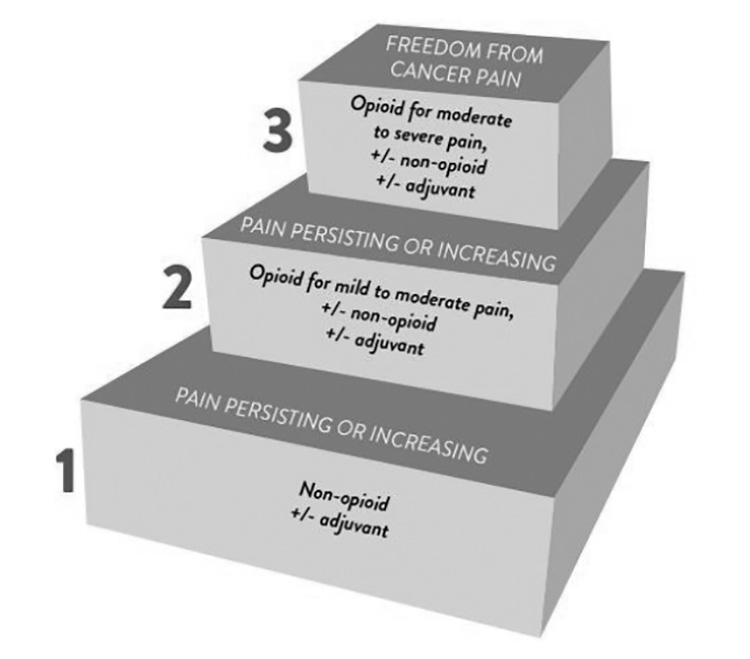
Which of the following is appropriate for mild pain, according to the WHO analgesic ladder?
Click to Review
- Back to Course Home
- Participation Instructions
- Review the course material online or in print.
- Complete the course evaluation.
- Review your Transcript to view and print your Certificate of Completion. Your date of completion will be the date (Pacific Time) the course was electronically submitted for credit, with no exceptions. Partial credit is not available.